Factor V Leiden 🦁 & Protein C/S deficiency 🐯 & VTE 🐻, oh my!
In this #tweetorial, we're going to tackle Thrombophilia & Anticoagulation
Thanks @_blake_smith for this week's edition
In this #tweetorial, we're going to tackle Thrombophilia & Anticoagulation
Thanks @_blake_smith for this week's edition
ICYMI
🎶catch Episode 47: Thrombophilia & Anticoagulation here: apple.co/2XhpRIU
In it, hematology expert Dr. Jean Connors @connors_md begins with a review of hemostasis🩸(coagulation)
🎶catch Episode 47: Thrombophilia & Anticoagulation here: apple.co/2XhpRIU
In it, hematology expert Dr. Jean Connors @connors_md begins with a review of hemostasis🩸(coagulation)

1⃣PRIMARY hemostasis:
initial vessel damage ➡️
exposure of sub-endothelial collagen ➡️
von Willebrand Factor (vWF) from ECs binds collagen ➡️
exposed vWF binds to GpIb receptor on platelets (plts) ➡️
plt adhesion! 💥
initial vessel damage ➡️
exposure of sub-endothelial collagen ➡️
von Willebrand Factor (vWF) from ECs binds collagen ➡️
exposed vWF binds to GpIb receptor on platelets (plts) ➡️
plt adhesion! 💥

plt adhesion is therefore specific to the site of injury, resulting in *local* accumulation of plts
binding of GpIb ➡️ plt release of ADP, Ca2+, thromboxane A2 (TXA2)
local ADP release ➡️ binding to neighboring P2Y12 receptors ➡️ GpIIb/IIIa expression on plts
why do I care? 🤷
binding of GpIb ➡️ plt release of ADP, Ca2+, thromboxane A2 (TXA2)
local ADP release ➡️ binding to neighboring P2Y12 receptors ➡️ GpIIb/IIIa expression on plts
why do I care? 🤷

GpIIb/IIIa receptors link together plts via a fibrinogen bridge 🔗🤝🔗 resulting in the famed 'platelet plug'
💊pharm interlude💊
1⃣Aspirin inhibits COX enzymes, blocking TXA2 synth.
2⃣Clopidogrel (Plavix) blocks P2Y12 (ADP) receptors
3⃣Abciximab inhibits GpIIb/IIIa receptors
💊pharm interlude💊
1⃣Aspirin inhibits COX enzymes, blocking TXA2 synth.
2⃣Clopidogrel (Plavix) blocks P2Y12 (ADP) receptors
3⃣Abciximab inhibits GpIIb/IIIa receptors

Cue every med student's favorite topic: coagulation cascade!
🟢Intrinsic pathway (aPTT): Factors 12, 11, 9, 8
🟣Extrinsic pathway (PT/INR): Factor 7
🔴Common pathway: Factors 10, 5, 2 (thrombin), 1 (fibrinogen) ➡️ fibrin mesh
together, this culminates in2⃣SECONDARY hemostasis
🟢Intrinsic pathway (aPTT): Factors 12, 11, 9, 8
🟣Extrinsic pathway (PT/INR): Factor 7
🔴Common pathway: Factors 10, 5, 2 (thrombin), 1 (fibrinogen) ➡️ fibrin mesh
together, this culminates in2⃣SECONDARY hemostasis

Before we move on to dysregulation of coagulation (hypercoaguability/thrombophilia), let's do a quick ⏰ quiz ✏️
Which components are involved in PRIMARY hemostasis?
Which components are involved in PRIMARY hemostasis?
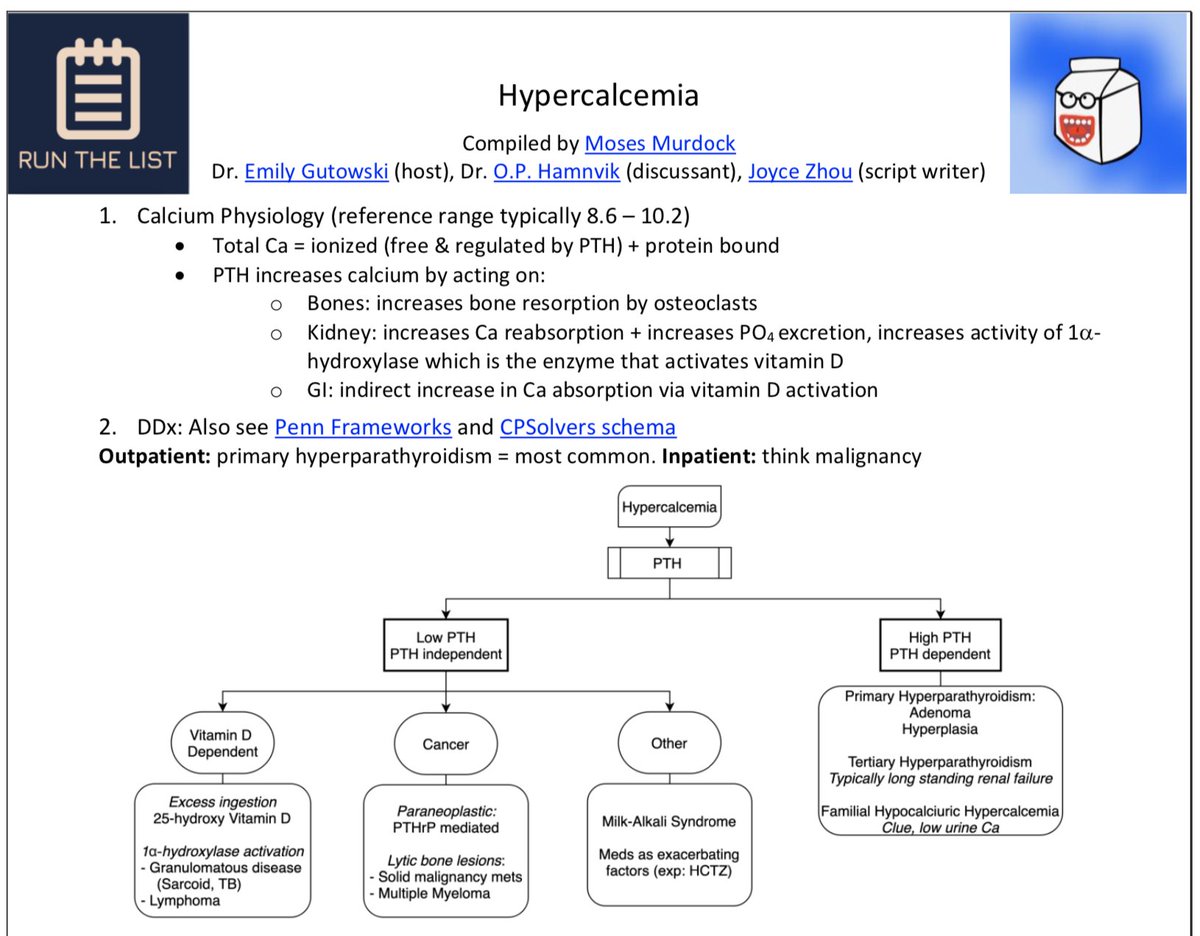
Now that we've established our hemostasis framework (meshwork?), let's talk about thrombophilia!
borrowing the schema from our RTL handout, we can break it down into 2 major buckets:
1⃣CONGENITAL
2⃣ACQUIRED
--
download handout (free!) here 👇runthelistpodcast.com/hematologyonco…
#FOAMed
borrowing the schema from our RTL handout, we can break it down into 2 major buckets:
1⃣CONGENITAL
2⃣ACQUIRED
--
download handout (free!) here 👇runthelistpodcast.com/hematologyonco…
#FOAMed
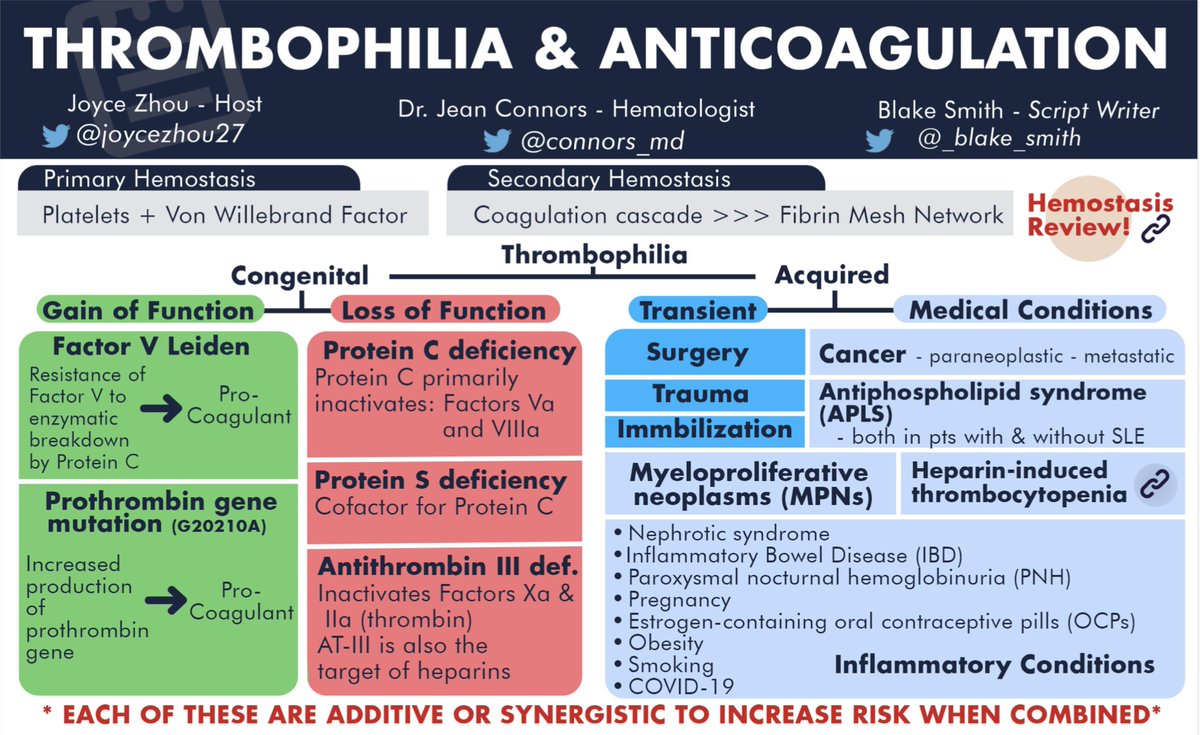
CONGENITAL causes can be subdivided:
GoF 👆
-Factor V Leiden (FVL)
-Prothrombin gene mutation (G20210A)
LoF 👇
-Protein C/S deficiency
-Antithrombin III deficiency (AT-III)
Regardless of the cause, *all* ➡️ PRO-coagulation
review from @connors_md on how (& when) to dx 👇
GoF 👆
-Factor V Leiden (FVL)
-Prothrombin gene mutation (G20210A)
LoF 👇
-Protein C/S deficiency
-Antithrombin III deficiency (AT-III)
Regardless of the cause, *all* ➡️ PRO-coagulation
review from @connors_md on how (& when) to dx 👇

There are many, many ACQUIRED causes of thrombophilia that we can't comprehensively cover, but to highlight a few:
-Trauma🩹, surgery, prolonged immobilization
-Cancer🦀 (metastatic, Trousseau's syndrome)
-Hematologic🩸(MPNs, PNH, HIT)
-Nephrotic syndrome (acq. AT-III def)
-Trauma🩹, surgery, prolonged immobilization
-Cancer🦀 (metastatic, Trousseau's syndrome)
-Hematologic🩸(MPNs, PNH, HIT)
-Nephrotic syndrome (acq. AT-III def)

Today, we'll focus on Factor V Leiden (FVL):
🔍quick facts🔎
1⃣FVL = CONGENITAL & common!
-present in up to 5% of Caucasian, 2% of Hispanic, & 1% of African-American populations
2⃣Arg506Gln mutation:
-replaces native cleavage site (R506) with an enzyme-resistant amino acid (Q)
🔍quick facts🔎
1⃣FVL = CONGENITAL & common!
-present in up to 5% of Caucasian, 2% of Hispanic, & 1% of African-American populations
2⃣Arg506Gln mutation:
-replaces native cleavage site (R506) with an enzyme-resistant amino acid (Q)

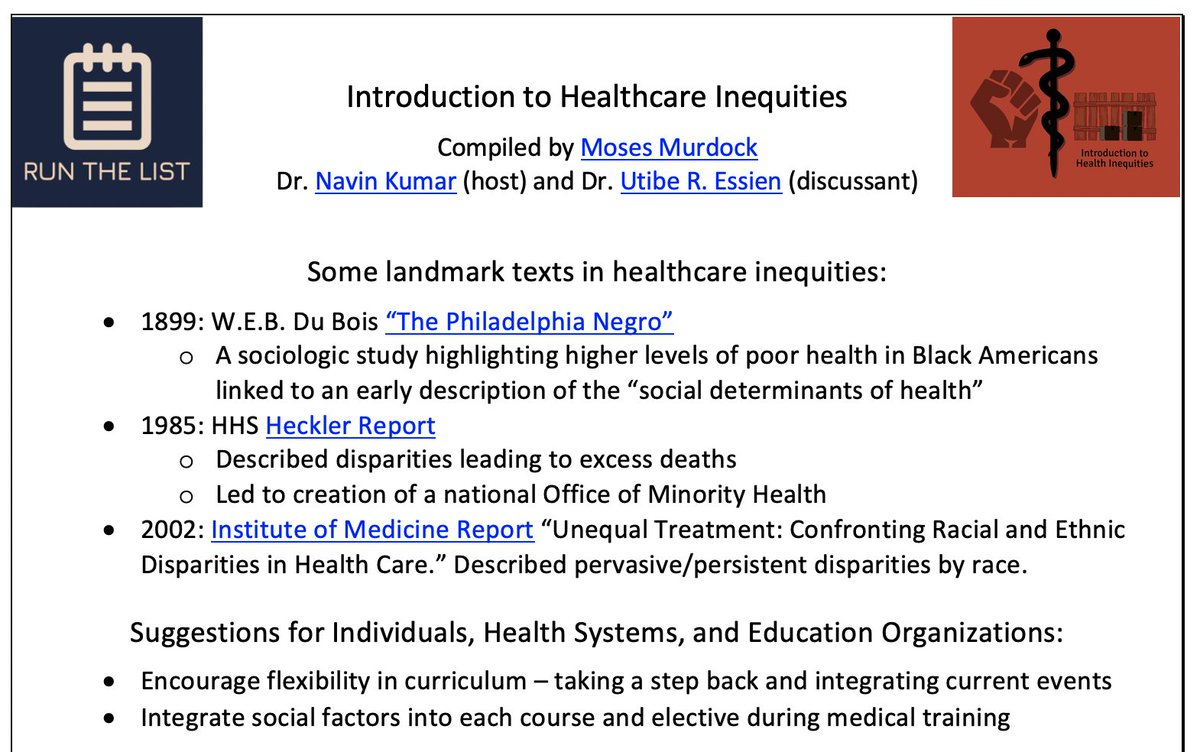
activated Protein C (aPC), together w/ cofactor Protein S, acts as a serine protease that cleaves at R506
w/ pathologic R506*Q mutation (FVL), this breakdown no longer occurs
risk of venous thromboembolism (VTE) in R506Q pts:
⬆️ 4-5x in heterozygotes
⬆️ 80x in homozygotes 🚨!
w/ pathologic R506*Q mutation (FVL), this breakdown no longer occurs
risk of venous thromboembolism (VTE) in R506Q pts:
⬆️ 4-5x in heterozygotes
⬆️ 80x in homozygotes 🚨!


Common VTE in FVL:
▪️DVT
▫️PE
Other vascular beds:
🔹Cerebral sinuses
🔸Portal, hepatic veins (Budd-Chiari)
Notably, risk of VTE in FVL can synergistically ⬆️ when combined w/ other causes of thrombophilia
As an example, FVL + oral contraceptive pills (OCP) ⬆️ risk of VTE 35x!
▪️DVT
▫️PE
Other vascular beds:
🔹Cerebral sinuses
🔸Portal, hepatic veins (Budd-Chiari)
Notably, risk of VTE in FVL can synergistically ⬆️ when combined w/ other causes of thrombophilia
As an example, FVL + oral contraceptive pills (OCP) ⬆️ risk of VTE 35x!

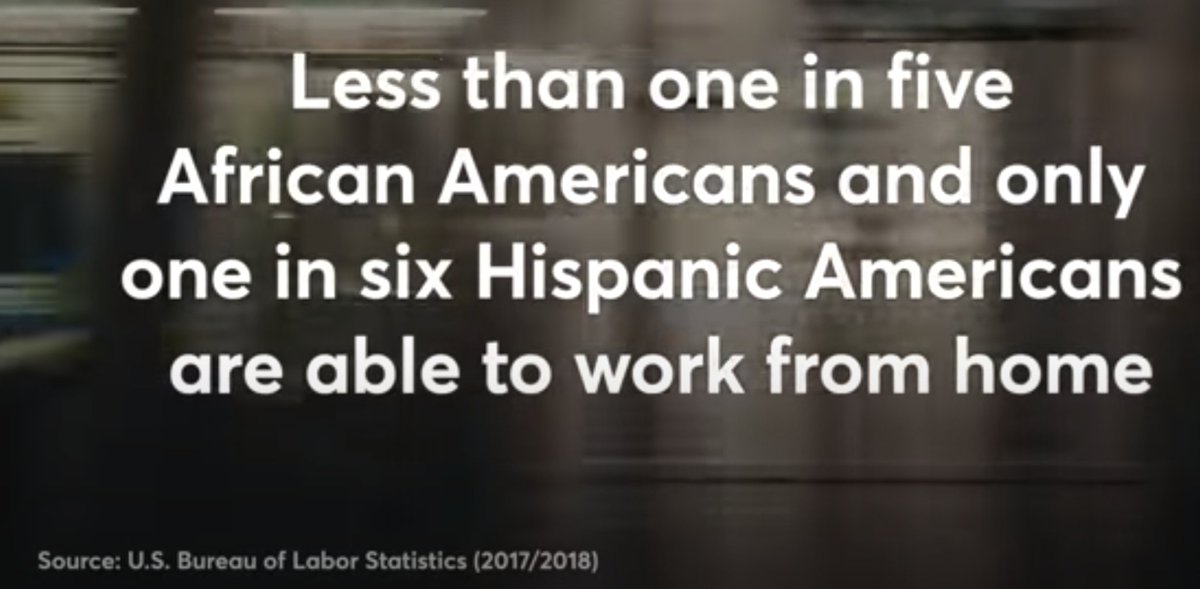
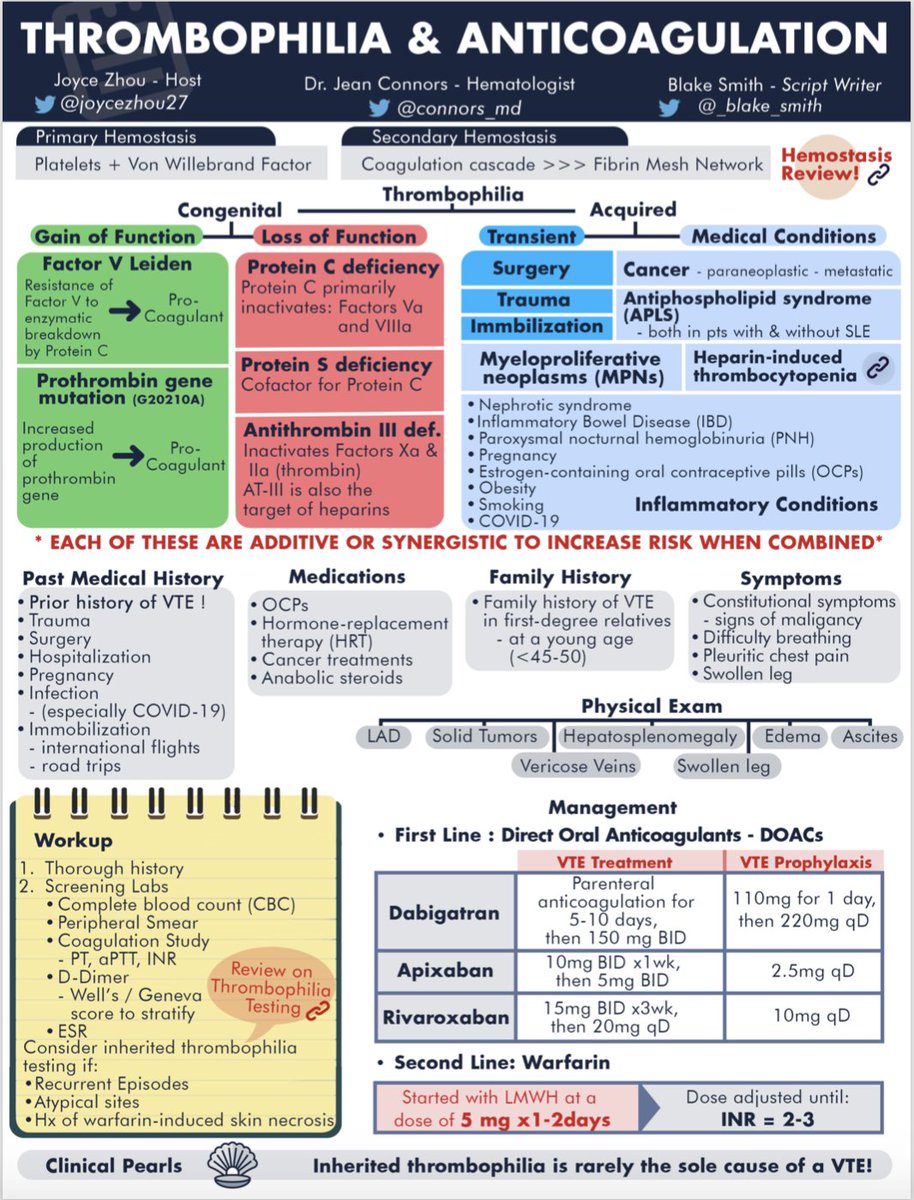
So... when do we dx FVL?
in general, testing is only indicated in pts with:
◾️strong family hx of VTE (first-relatives)
◽️young age (<50 yo)
◾️atypical vascular bed (e.g. mesenteric vein)
◽️unusually recurrent VTE
in general, testing is only indicated in pts with:
◾️strong family hx of VTE (first-relatives)
◽️young age (<50 yo)
◾️atypical vascular bed (e.g. mesenteric vein)
◽️unusually recurrent VTE

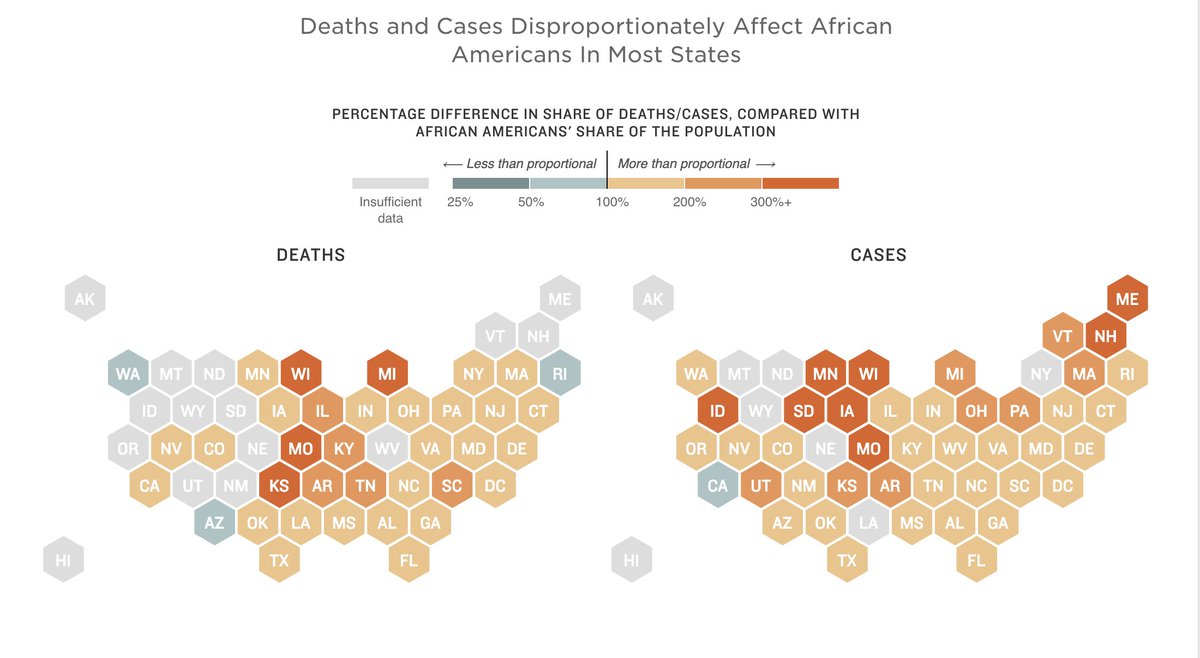
Once testing is considered, there are 2 main tests:
1⃣functional assay: aPC resistance (APCR); aPTT fails to prolong after mixing with normal aPC
2⃣genetic testing: detection of single nucleotide polymorphism (SNP: G1691A -> R506Q) from peripheral blood cells
1⃣functional assay: aPC resistance (APCR); aPTT fails to prolong after mixing with normal aPC
2⃣genetic testing: detection of single nucleotide polymorphism (SNP: G1691A -> R506Q) from peripheral blood cells


As with all causes of thrombophilia, 🩹 tx of FVL is complex (depends on pt age, clinical course, gene status, other causes of coag, etc), but largely consists of:
💊DOACs (dabigatran, rivaroxaban, apixaban) or
💊Warfarin + LMWH or fondaparinux bridge (w/ INR monitoring)
💊DOACs (dabigatran, rivaroxaban, apixaban) or
💊Warfarin + LMWH or fondaparinux bridge (w/ INR monitoring)

IN SUM
🔹Coagulation = 1 (plt plug) & 2 (coag cascade+fibrin mesh) hemostasis
🔸Thrombophilia is both congenital & acq.
🔹Congenital causes: FVL, Prothrombin, Prot C/S def, AT-III def
🔸Acquired causes: Obesity, smoking, cancer, OCP, etc.
🔹FVL⬆️VTE risk, Tx: DOACs, Warfarin
🔹Coagulation = 1 (plt plug) & 2 (coag cascade+fibrin mesh) hemostasis
🔸Thrombophilia is both congenital & acq.
🔹Congenital causes: FVL, Prothrombin, Prot C/S def, AT-III def
🔸Acquired causes: Obesity, smoking, cancer, OCP, etc.
🔹FVL⬆️VTE risk, Tx: DOACs, Warfarin
REFs 1:
[3] nejm.org/doi/full/10.10…
[4] what-when-how.com/acp-medicine/h…
[5] ahajournals.org/doi/full/10.11…
[6] stepwards.com/?page_id=866
[9] nejm.org/doi/full/10.10…
[10] link.springer.com/chapter/10.100…
[11a] uptodate.com/contents/facto…
[11b] what-when-how.com/acp-medicine/t…
[12]
[3] nejm.org/doi/full/10.10…
[4] what-when-how.com/acp-medicine/h…
[5] ahajournals.org/doi/full/10.11…
[6] stepwards.com/?page_id=866
[9] nejm.org/doi/full/10.10…
[10] link.springer.com/chapter/10.100…
[11a] uptodate.com/contents/facto…
[11b] what-when-how.com/acp-medicine/t…
[12]
REFs 2:
[13] cyberleninka.org/article/n/1038…
[14] nejm.org/doi/full/10.10…
[15a] nejm.org/doi/full/10.10…
[15b] ahajournals.org/doi/10.1161/01…
[16] ahajournals.org/doi/full/10.11…
[13] cyberleninka.org/article/n/1038…
[14] nejm.org/doi/full/10.10…
[15a] nejm.org/doi/full/10.10…
[15b] ahajournals.org/doi/10.1161/01…
[16] ahajournals.org/doi/full/10.11…

@MedTweetorials @CPSolvers @COREIMpodcast @CuriousClinPod @DxRxEdu @rabihmgeha @tony_breu @AvrahamCooperMD @medrants @connors_md @DavidSteensma
• • •
Missing some Tweet in this thread? You can try to
force a refresh