
Prof Darrel Francis ☺ Mk CardioFellows Great Again
1 Nov,
60 tweets, 11 min read
Josh isn't the first person to think of this, merely the last. 

Why don't we have such studies?
Who does studies like that? RCTs?
What do all people who do RCTs have in common?
And when you plan a trial, you have to decide first what the endpoint is, and with that in mind, you can decide how many people need to participate, for it not to be a gigantic waste of time.
What would you have as the endpoint?
What would you have as the endpoint?
I notice the MASSIVE dropoff in answering from the previous question to this latest one!
8-)
At least it has given people pause for thought.
8-)
At least it has given people pause for thought.
That is an interesting study but is testing INDIVIDUAL randomization.
Which does that test?
Which does that test?
Because people are randomized individually, the study tests whether the INDIVIDUALS get infected, i.e. whether the masks protect the WEARER.
It CANNOT test whether masks prevent wearers infecting OTHERS - which is why I wear my mask.
It CANNOT test whether masks prevent wearers infecting OTHERS - which is why I wear my mask.
How could you test whether masks protect OTHERS, not the wearers?
("Outbound protection", rather than the "Inbound protection" that the Danish study is testing)
("Outbound protection", rather than the "Inbound protection" that the Danish study is testing)
I really, really hope nobody is dim enough to vote for randomise non-participants.
It doesn't even mean anything!
"It's not even wrong," as they say!
It doesn't even mean anything!
"It's not even wrong," as they say!
You can't randomize people who are NOT participating in the study. If you randomize them, they are participating!
So you have to randomize communities, and hope to pick up a change in proportion, of whatever endpoint you went for.
Death was a popular endpoint.
Death was a popular endpoint.
Let's say overall mortality from infection (asymptomatic or symptomatic) is 1% (I know I am over-stating it, but it is to be generous).
And let's say we can get in to a community with 10% of people already having had Corona.
And we run the study until (say) 30% get it.
And let's say we can get in to a community with 10% of people already having had Corona.
And we run the study until (say) 30% get it.
What proportion of people in the community would we be expecting to get Corona, while the study runs?
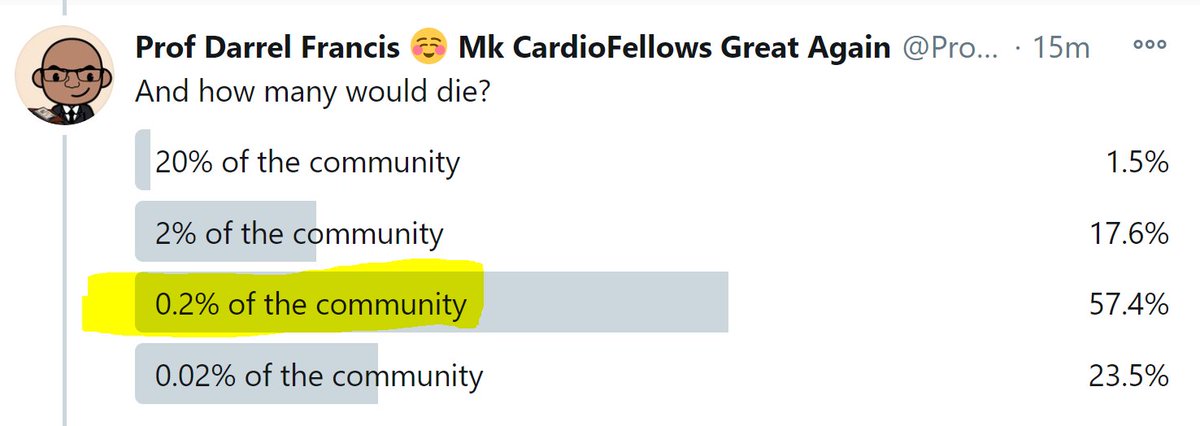
And how many would die?
Now let's look at how weak a mask effect we would be needing to test for.
Imagine if when living your ordinary life, if you got covid and didn't wear a mask, you would infect an average of 1.5 people with Covid.
Imagine if when living your ordinary life, if you got covid and didn't wear a mask, you would infect an average of 1.5 people with Covid.
Someone suggests you wear a mask to reduce that transmission to others. You ask "How much would it reduce it to?"
At what answer would you say "That's too feeble an effect, I will not wear a mask for just that"
At what answer would you say "That's too feeble an effect, I will not wear a mask for just that"
Me too, I would lose interest at 1.49, i.e. ~1% relative risk reduction.
Remember that is a ~1% reduction in ALL THE PEOPLE I KILL by merrily transmitting my corona virus to a chain of other people.
Remember that is a ~1% reduction in ALL THE PEOPLE I KILL by merrily transmitting my corona virus to a chain of other people.
Different people will have different thresholds.
If we design a trial that can only detect a reduction from 1.5 to (say) 1.3, then it may result in "No, the mask did not reduce transmission to 1.3"
... and all the "1.45" or "1.49"ers will be up in arms.
If we design a trial that can only detect a reduction from 1.5 to (say) 1.3, then it may result in "No, the mask did not reduce transmission to 1.3"
... and all the "1.45" or "1.49"ers will be up in arms.
"What a tremendous waste of time! Nobody seriously expected masks to slash infection that much! We only expect it to slice 1 or 2% of outbound infections!"
So the trial has failed - mask believers continue to believe, and anti-maskers stay anti-maskers.
So the trial has failed - mask believers continue to believe, and anti-maskers stay anti-maskers.
Therefore we should design the trial to be able to detect quite a small reduction in outbound infection, e.g. from 1.50 to 1.47.
Let's describe that as a Weakness factor, for the weakness of the effect.
Let's describe that as a Weakness factor, for the weakness of the effect.
A reduction from 1.50 to 1.47 is a reduction of 0.03 downstream infected people, per 1.50 that would normally get infected.
0.03 in 1.50 is what fraction?
0.03 in 1.50 is what fraction?
Meanwhile, the Wisdom of the Crowd has correctly calculated how RARE the endpoint is.
"Dying of Corona" occurs in this proportion of the population.
"Dying of Corona" occurs in this proportion of the population.
Let's describe this as a fraction.
The Corona deaths during the trial are what fraction of the entire community?
The Corona deaths during the trial are what fraction of the entire community?
Here comes the science bit.
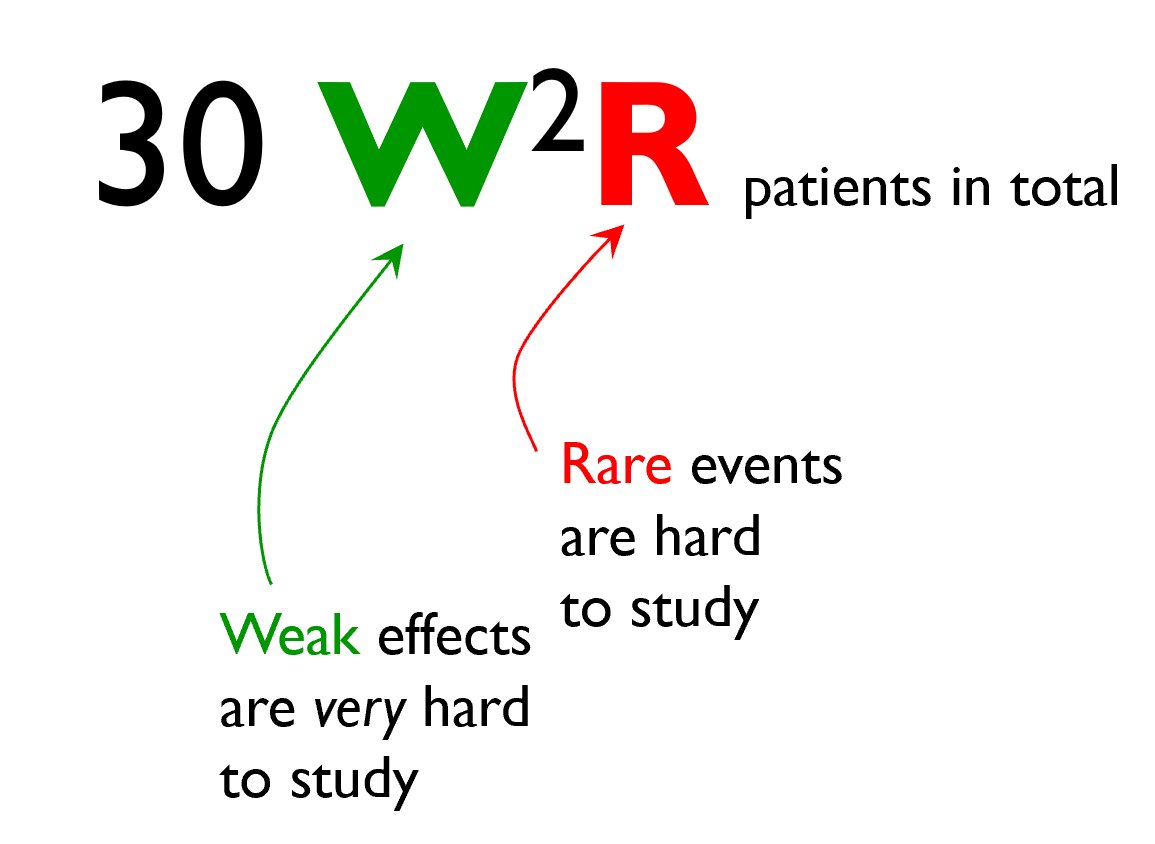
If you can define the RARENESS of the endpoint, as "1 in R"
and the WEAKNESS of the intervention, as "1 in W", to mean that of every W events that would have happened, by wearing a mask you can prevent 1.
The sample size you need is:
If you can define the RARENESS of the endpoint, as "1 in R"
and the WEAKNESS of the intervention, as "1 in W", to mean that of every W events that would have happened, by wearing a mask you can prevent 1.
The sample size you need is:
If any journal editor out there wants us to publish the explanation of this, just let me know on d.francis@imperial.ac.uk
A couple that we submitted our methods paper to, said "Everyone knows this", which differs from my experience, but we got bored with trying.
A couple that we submitted our methods paper to, said "Everyone knows this", which differs from my experience, but we got bored with trying.
You have already derived that:
[R]arity of event = 500
[W]eakness of intervention = 50
What is the sample size required?
30 W^2 R
[R]arity of event = 500
[W]eakness of intervention = 50
What is the sample size required?
30 W^2 R
That's assuming that everyone in each arm does what you tell them to do
In reality, I am not going to agree to de-mask, just because somebody says "London - you guys de-mask"
And there will be people in, say, Birmingham who refuse to mask because someone tells the city to mask.
In reality, I am not going to agree to de-mask, just because somebody says "London - you guys de-mask"
And there will be people in, say, Birmingham who refuse to mask because someone tells the city to mask.
If you try to randomize whole cities like this, let's guess that
30% continue to mask anyway
30% continue to non-mask
and 10% participate in the request to mask or non-mask
(I still think that is overestimating the agree-ers)
30% continue to mask anyway
30% continue to non-mask
and 10% participate in the request to mask or non-mask
(I still think that is overestimating the agree-ers)
So NOW what is the weakness of therapy?
Instead of preventing 1 in 50 infections, what proportion can we prevent if only 1/10 of the population mask/demask differently between the trial arms?
Instead of preventing 1 in 50 infections, what proportion can we prevent if only 1/10 of the population mask/demask differently between the trial arms?
Oh deary deary me.

R = 500
W = 500
W = 500
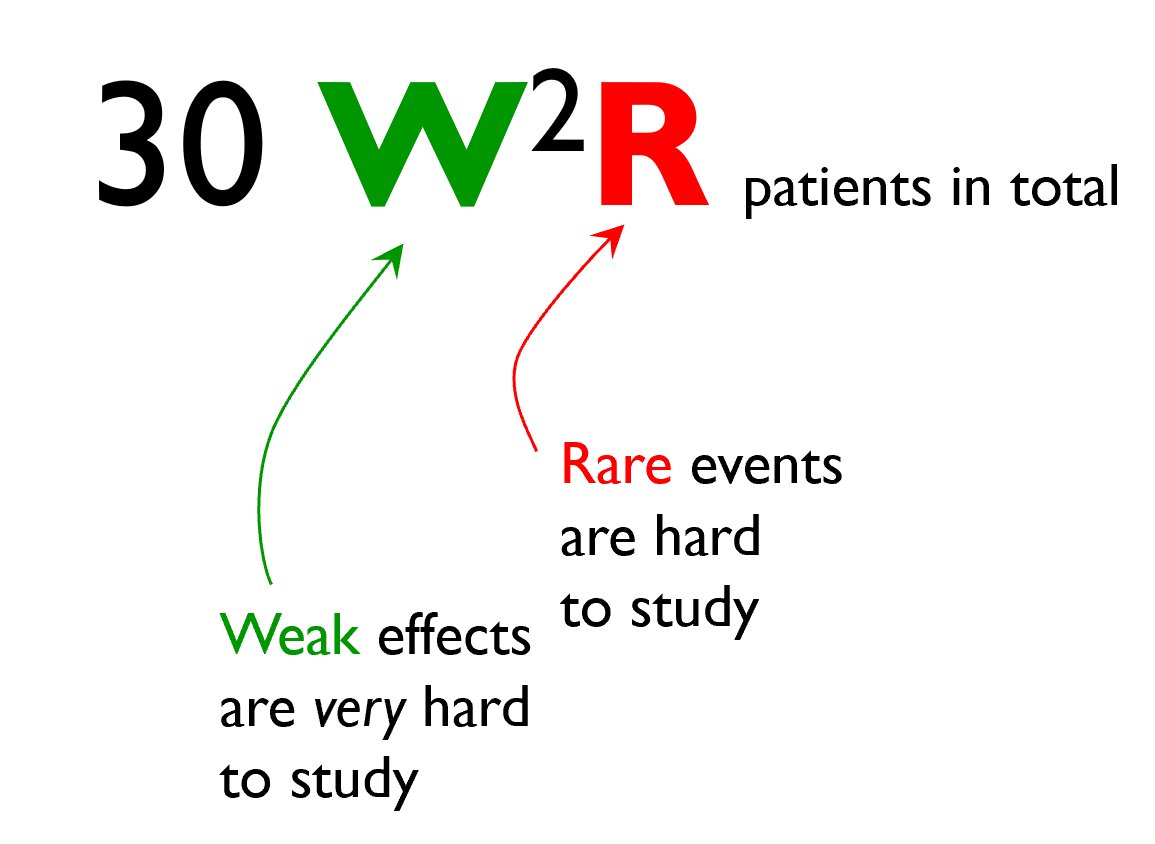
How many people do we need now?
And THAT is why these first 3 answers are all wrong.
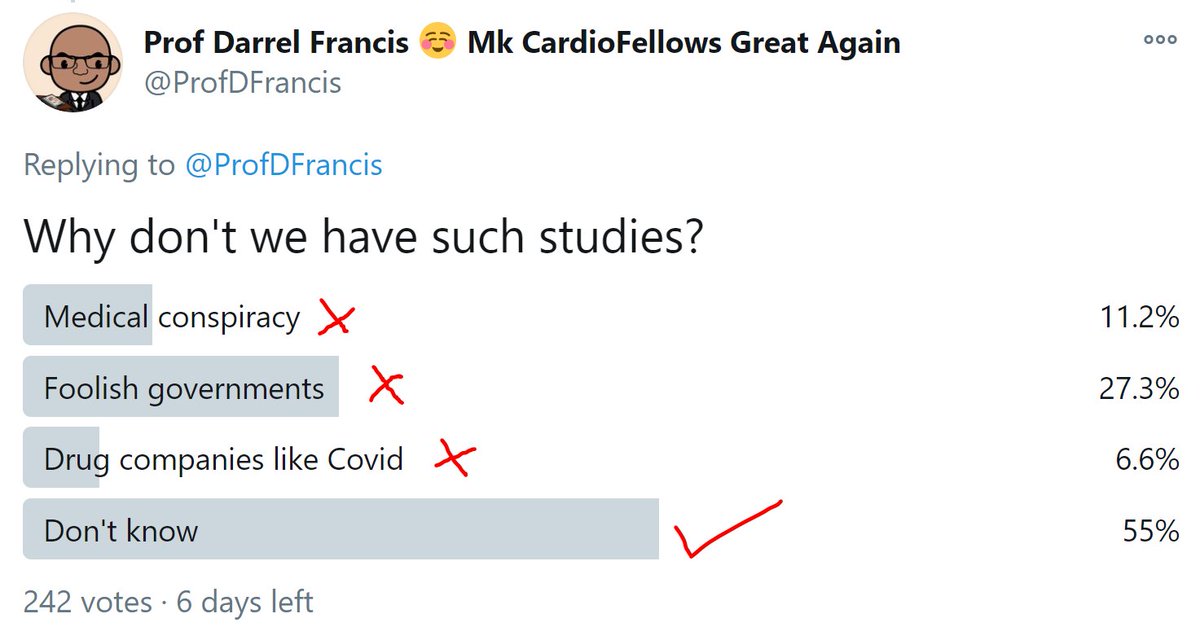
Scientists and even governments (although sometimes it is hard to believe it) are composed of experts who have to think carefully about what they do.
People can randomly say any old shit, but experts are more careful.
They don't always explain, because they think the average person is too stupid to understand.
I am more optimistic and make the effort, because I think people can understand if you explain patiently.
They don't always explain, because they think the average person is too stupid to understand.
I am more optimistic and make the effort, because I think people can understand if you explain patiently.
For more chitchat about Statistical Thinking for Medics (and people interested in Medical stuff), see this online annoy-a-arama which is developing week-by-week based on feedback:
No module takes more than 15 min.
Currently accessible free.
Click→ inspirion.org/sc/aca~-MDQ9cX…
No module takes more than 15 min.
Currently accessible free.
Click→ inspirion.org/sc/aca~-MDQ9cX…

Good point raised here.
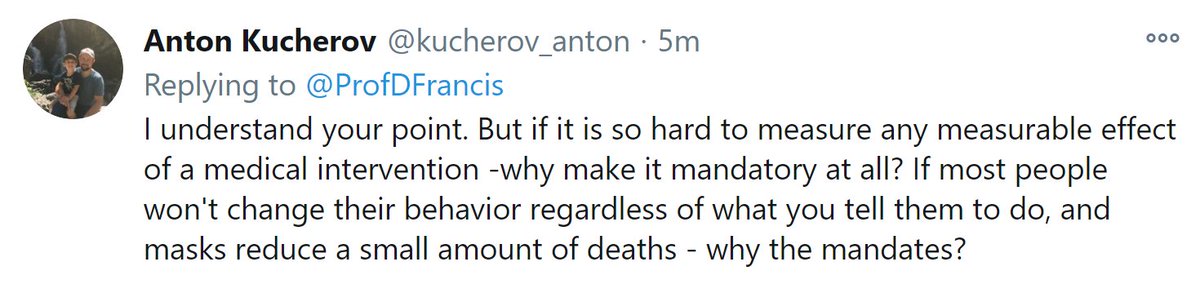
Why enforce a mandate without evidence?
The same reason we have speed limits around schools.
Not to protect the drivers!
And not because we have RCTs of reduction in child deaths.
It is because the inconvenience of the mandate is small compared to the guessed benefit.
The same reason we have speed limits around schools.
Not to protect the drivers!
And not because we have RCTs of reduction in child deaths.
It is because the inconvenience of the mandate is small compared to the guessed benefit.
For masks, the cost is very low, compared to the cost of locking down a city.
While government employees like me are fine, and keep earning their salary, people who actually have to do real hard work for a living, can no longer run their shops, cut people's hair, etc.
While government employees like me are fine, and keep earning their salary, people who actually have to do real hard work for a living, can no longer run their shops, cut people's hair, etc.
And even selfishly, future taxpayers (like me) will have to foot the bill for all the financial misery caused. That bill is much more trivial than the actual misery for the people unable to work, but at least even selfish people can see why it is bad.
Through taxes or inflation.
Through taxes or inflation.
So anything we can do to slow the spread, that doesn't throw people out of their livelihood when they would otherwise be keen to work (and even enjoy working and enjoy being good at their work!) would be worth doing if it is not too much trouble.
Social distancing is a bit troublesome. Every extra 10cm gap imposed causes people to dangle into the street etc when queueing, or fewer people fit into a shop or restaurant.
But we still do it.
Masking is much less troublesome.
So let's do it and stop talking about it.
But we still do it.
Masking is much less troublesome.
So let's do it and stop talking about it.
Great way to put it! Haha
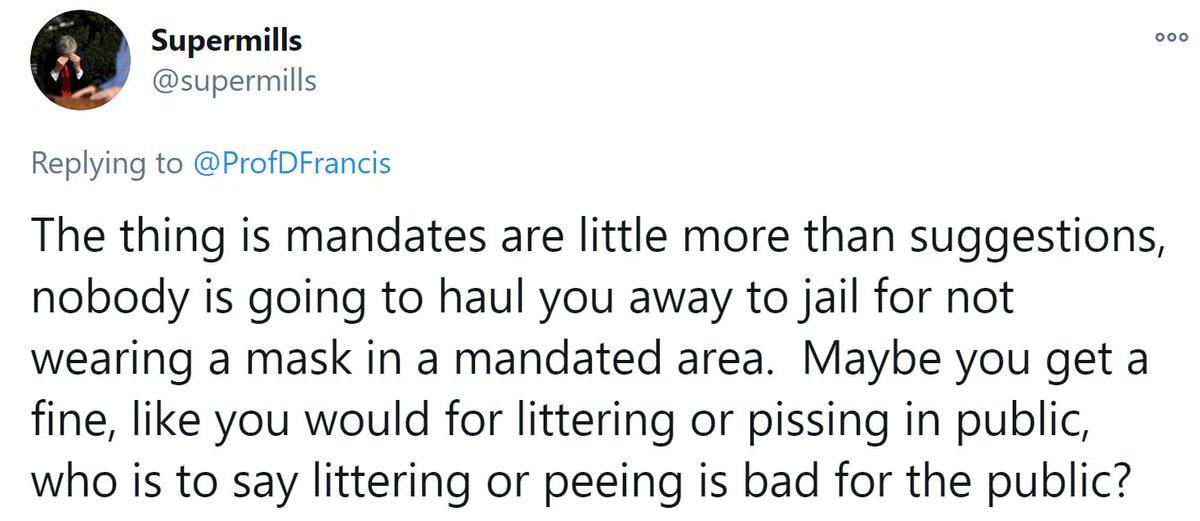
Exactly!
If I throw an apple core onto some grass, the police COULD do me for littering, when in fact it is a perfectly biodegradable thing and it is more eco-friendly to do that than throw it in a bin where it needs to be collected and moved to landfill.
If I throw an apple core onto some grass, the police COULD do me for littering, when in fact it is a perfectly biodegradable thing and it is more eco-friendly to do that than throw it in a bin where it needs to be collected and moved to landfill.
But the police won't actually bother.
People will just give me a hard stare.
People will just give me a hard stare.

And they won't arrest me for non-masking.
Unless there are people who are around me who are getting scared by my non-maskedness and complain.
But still they will probably just tell me to go away from people, and if I did, they would lose interest. They have better things to do.
Unless there are people who are around me who are getting scared by my non-maskedness and complain.
But still they will probably just tell me to go away from people, and if I did, they would lose interest. They have better things to do.
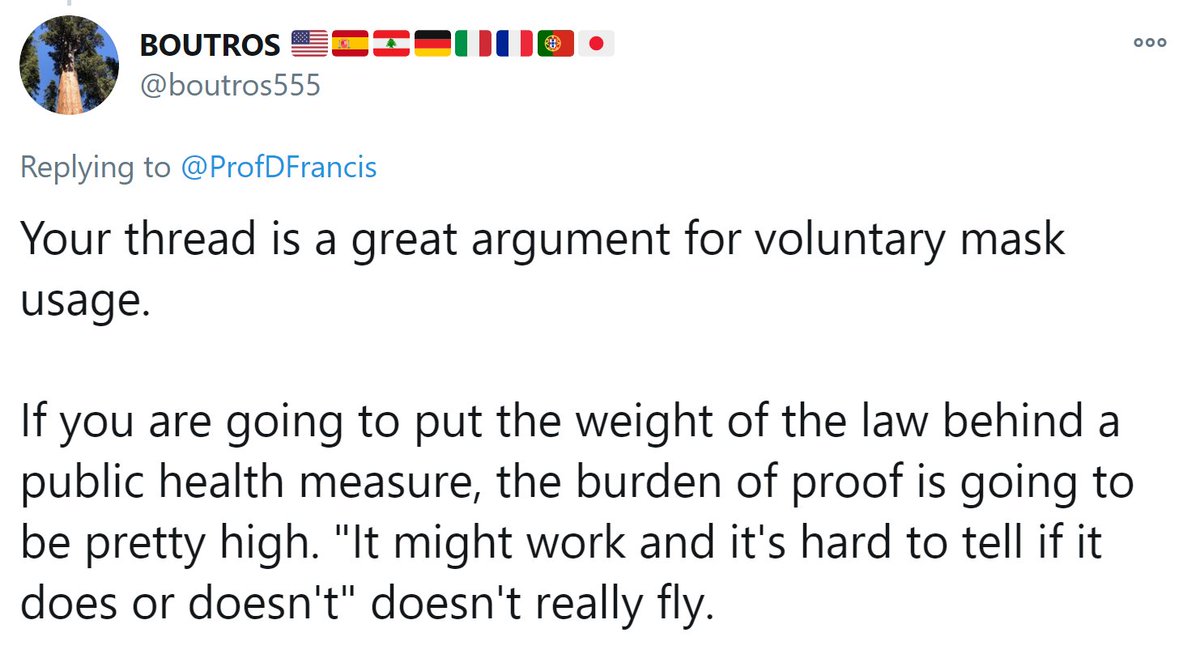
We don't really need a high burden of proof.
We don't have RCT evidence of passive smoking being dreadful, but we believe it must be *a bit* bad at least. That is the basis of telling smokers to sod off into the rain to smoke.
"No 2 metres for you!"
We don't have RCT evidence of passive smoking being dreadful, but we believe it must be *a bit* bad at least. That is the basis of telling smokers to sod off into the rain to smoke.
"No 2 metres for you!"
That's a law.
People don't moan about it on Twitter.
They just grumble and stand in the rain with their soggy cig.
I suggest mask-deniers just do that. It's a small ask.
It's like an expectation to bathe occasionally. Once a week (even if you don't need it!)
People don't moan about it on Twitter.
They just grumble and stand in the rain with their soggy cig.
I suggest mask-deniers just do that. It's a small ask.
It's like an expectation to bathe occasionally. Once a week (even if you don't need it!)
1. "To slow the pread": Does it?
From first principles I believe it must do (see the thing about the layers of T-shirt, above)
I can't argue it is a big reduction, but unless NO water particles are caught in the mask, there must be SOME reduction
Does your mask NEVER go moist?
From first principles I believe it must do (see the thing about the layers of T-shirt, above)
I can't argue it is a big reduction, but unless NO water particles are caught in the mask, there must be SOME reduction
Does your mask NEVER go moist?
2. "Doesn't throw people out of their livelihood": Forcing masks definitely drives some people away from businesses. Food hospitality for example.
Do you mean that some people won't go to a restaurant because they refuse to wear a mask in the street on the way in?
Do you mean that some people won't go to a restaurant because they refuse to wear a mask in the street on the way in?
If so, it is those people who are doing the throwing-people-out-of-work.
For my part, I went to a restaurant wearing a mask last night.
Very nice it was too!
hankies.london
For my part, I went to a restaurant wearing a mask last night.
Very nice it was too!
hankies.london

"Not too much trouble" : For some it's too much.
Yes. It is up to society to gauge how much effort an intervention is (for people in general).
For example, some people won't go places because they can't smoke there, or they can't bring their (non-guide) dog with them.
Yes. It is up to society to gauge how much effort an intervention is (for people in general).
For example, some people won't go places because they can't smoke there, or they can't bring their (non-guide) dog with them.
I suspect it is because we in the developed world have not suffered a (local) war or environmental catastrophe recently.
So we are busy thinking about our individual rights and freedoms, rather than a societal consequence.
So we are busy thinking about our individual rights and freedoms, rather than a societal consequence.
I suspect we have had more democracy than we would have been willing to earn through diligent study of decision-making.
For all who wish to invest in their own statistical thinking, may I plug our course?
Click→inspirion.org/sc/aca~-MDQ9cX…
For all who wish to invest in their own statistical thinking, may I plug our course?
Click→inspirion.org/sc/aca~-MDQ9cX…

Here is another good question.
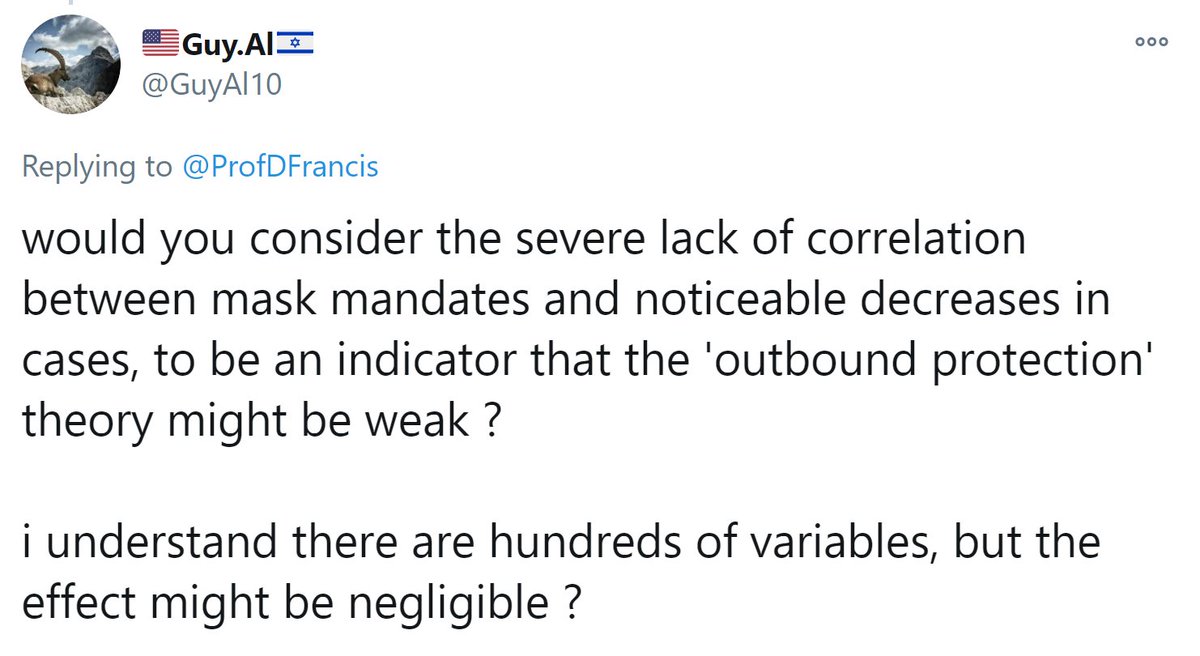
It is good that people are thinking about this, but remember the statistics of correlation?
How much would the effect have to be, and how complete would the changeover from non-mask to mask have to be, for the effect to be detectable in a country?
Worth doing the maths of it!
How much would the effect have to be, and how complete would the changeover from non-mask to mask have to be, for the effect to be detectable in a country?
Worth doing the maths of it!
• • •
Missing some Tweet in this thread? You can try to
force a refresh










