We are currently doing what could be the closest we can get to an RCT of restrictions and mandates: North vs. South Dakota. Two very similar states, but as of last Friday, very different policies in how they approach COVID. (1/x)
On Friday, ND imposed restrictions on bars and indoor dining, indoor events, and sports. They also mandated masks. Meanwhile, SD is not changing their approach and avoiding such restrictions. Here is a look at their cases so far (source for data is CTP): (2/x) 
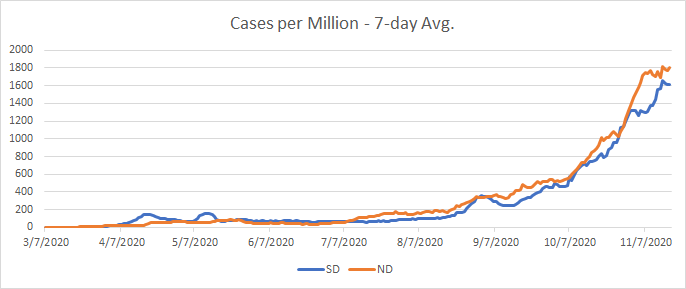
Their curves are very similar, so they are starting from the same place. We will soon know if they diverge as a result of ND's interventions. However, it is important to note that they are on slightly different latitudes, so there is that. Here is hospitalizations: (3/x)
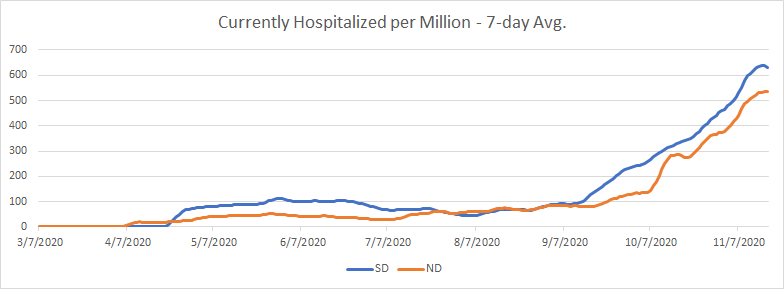
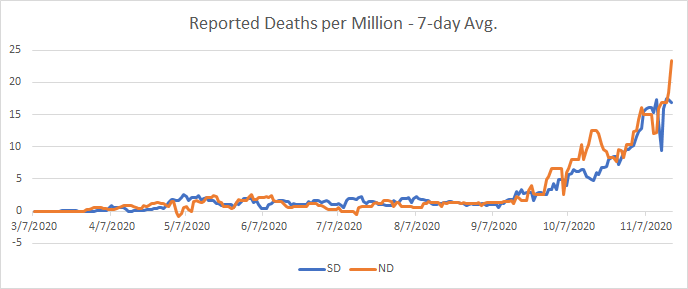
Finally, their reported deaths are also almost identical other than some small up/down swings. I will update these charts once every few days to see where we are and how the quasi-experiment is going. (4/4)
• • •
Missing some Tweet in this thread? You can try to
force a refresh