1/
Why does obesity cause a "falsely low" B-type natriuretic peptide (BNP) in patients with heart failure?
I often hear this used to explain unexpectedly low BNP results, but I've never really understood why.
Let's explore in a #tweetorial.
#medtwitter #cardiotwitter
Why does obesity cause a "falsely low" B-type natriuretic peptide (BNP) in patients with heart failure?
I often hear this used to explain unexpectedly low BNP results, but I've never really understood why.
Let's explore in a #tweetorial.
#medtwitter #cardiotwitter

2/
Before we answer this question, a quick poll.
What is the main physiologic mechanism of BNP?
Before we answer this question, a quick poll.
What is the main physiologic mechanism of BNP?
3/
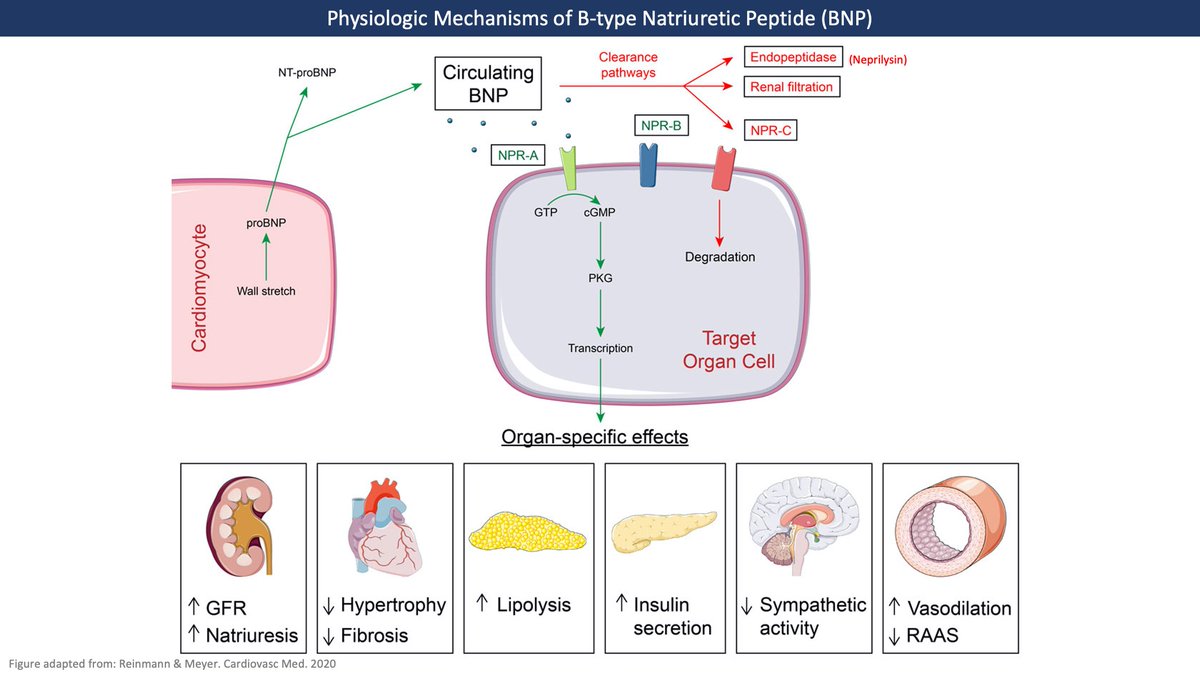
BNP is a hormone secreted in response to ventricular wall stretch. It binds to natriuretic peptide receptor A (NPR-A) which ⬆️ cGMP in various tissues to exert MANY effects including:
⬆️ Natriuresis
⬇️ RAAS
⬇️ sympathetic tone
& so much more!
cardiovascmed.ch/article/doi/cv…
BNP is a hormone secreted in response to ventricular wall stretch. It binds to natriuretic peptide receptor A (NPR-A) which ⬆️ cGMP in various tissues to exert MANY effects including:
⬆️ Natriuresis
⬇️ RAAS
⬇️ sympathetic tone
& so much more!
cardiovascmed.ch/article/doi/cv…
4/
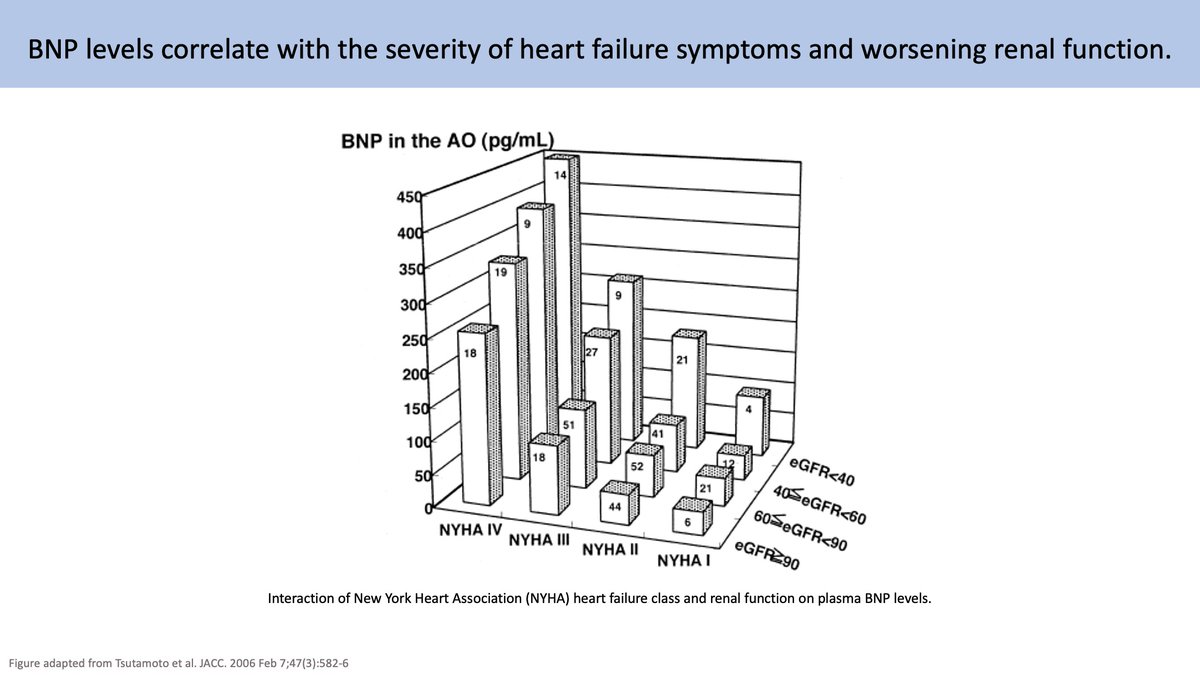
As ventricular overload ⬆️, so does transcription of BNP, which may explain why ⬆️ BNP levels correlate with worsening heart failure symptoms.
Transcription takes time though, so BNP may initially be low in acute events like flash pulmonary edema.
pubmed.ncbi.nlm.nih.gov/16291870/
As ventricular overload ⬆️, so does transcription of BNP, which may explain why ⬆️ BNP levels correlate with worsening heart failure symptoms.
Transcription takes time though, so BNP may initially be low in acute events like flash pulmonary edema.
pubmed.ncbi.nlm.nih.gov/16291870/
5/
The clearance of BNP occurs via three main mechanisms:
1️⃣ Binding to NPR-C - a clearance receptor that leads to liposomal degradation.
2️⃣ Renal filtration
3️⃣ Cleavage by various endopeptidases such as neprilysin
🔑 These will be important to our discussion later.
The clearance of BNP occurs via three main mechanisms:
1️⃣ Binding to NPR-C - a clearance receptor that leads to liposomal degradation.
2️⃣ Renal filtration
3️⃣ Cleavage by various endopeptidases such as neprilysin
🔑 These will be important to our discussion later.
6/
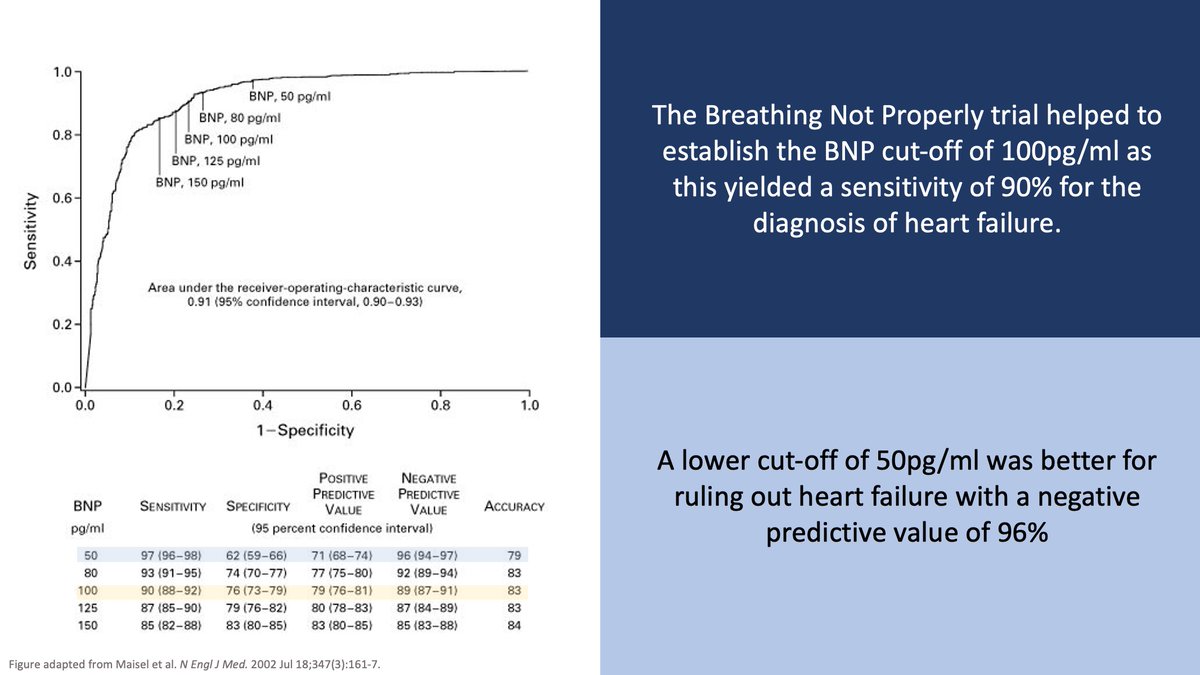
With the advent of BNP assays in the 1990s came studies validating the use of BNP to diagnose heart failure.
The Breathing Not Properly trial found a cut-off of 100 pg/ml was 90% sensitive and 76% specific for diagnosing heart failure.
pubmed.ncbi.nlm.nih.gov/12124404/
With the advent of BNP assays in the 1990s came studies validating the use of BNP to diagnose heart failure.
The Breathing Not Properly trial found a cut-off of 100 pg/ml was 90% sensitive and 76% specific for diagnosing heart failure.
pubmed.ncbi.nlm.nih.gov/12124404/
7/
It soon became apparent, however, that BNP levels were influenced by several other factors.
▪️ Age, hypertension, and kidney disease correlated with higher BNP levels
▪️ Obesity correlated with lower BNP levels.
pubmed.ncbi.nlm.nih.gov/12807847/
pubmed.ncbi.nlm.nih.gov/14769680/
It soon became apparent, however, that BNP levels were influenced by several other factors.
▪️ Age, hypertension, and kidney disease correlated with higher BNP levels
▪️ Obesity correlated with lower BNP levels.
pubmed.ncbi.nlm.nih.gov/12807847/
pubmed.ncbi.nlm.nih.gov/14769680/

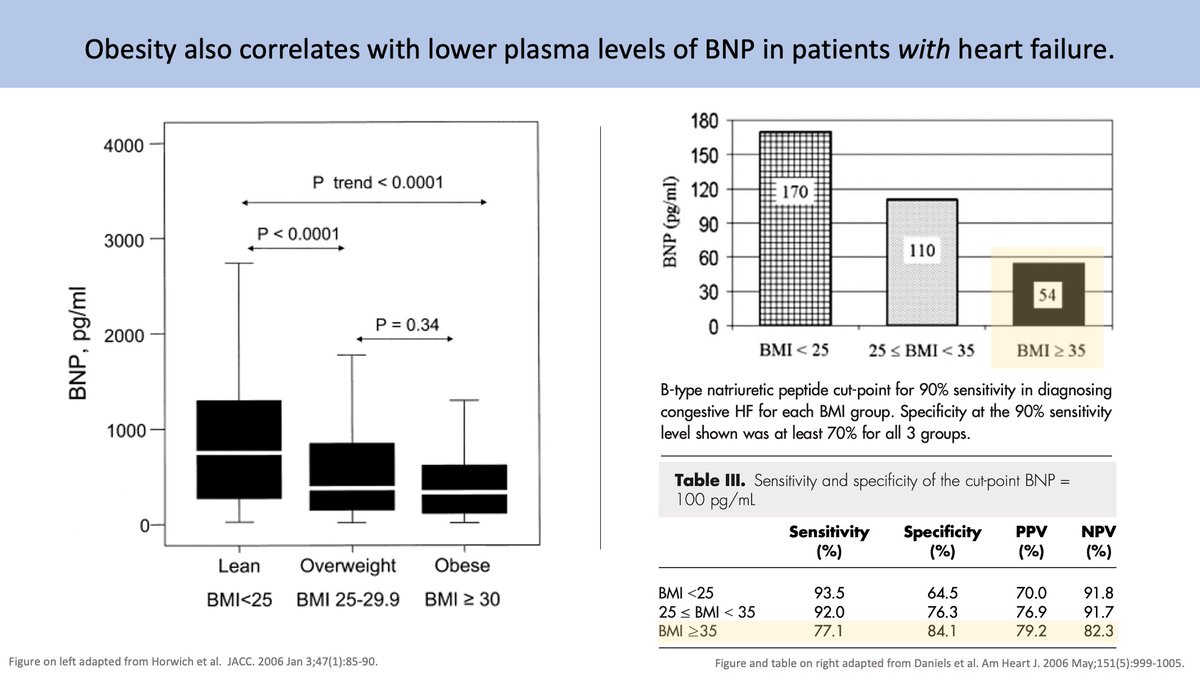
8/
These findings were corroborated in heart failure patients who also had ⬇️ BNP values with ⬆️ BMI.
In fact, the 100pg/ml cut-off was only 77% sensitive for diagnosing CHF in patients with BMI ≥35.
pubmed.ncbi.nlm.nih.gov/16386669/
pubmed.ncbi.nlm.nih.gov/16644321/ 🔒
These findings were corroborated in heart failure patients who also had ⬇️ BNP values with ⬆️ BMI.
In fact, the 100pg/ml cut-off was only 77% sensitive for diagnosing CHF in patients with BMI ≥35.
pubmed.ncbi.nlm.nih.gov/16386669/
pubmed.ncbi.nlm.nih.gov/16644321/ 🔒
9/
So we know there is an inverse correlation between BMI & BNP.
Is there a potential mechanism to explain this?
The answer isn't fully understood but the answer may lie in how obesity impacts all three BNP clearance mechanisms:
1️⃣ NPR-C
2️⃣ Renal filtration
3️⃣ Neprilysin
So we know there is an inverse correlation between BMI & BNP.
Is there a potential mechanism to explain this?
The answer isn't fully understood but the answer may lie in how obesity impacts all three BNP clearance mechanisms:
1️⃣ NPR-C
2️⃣ Renal filtration
3️⃣ Neprilysin
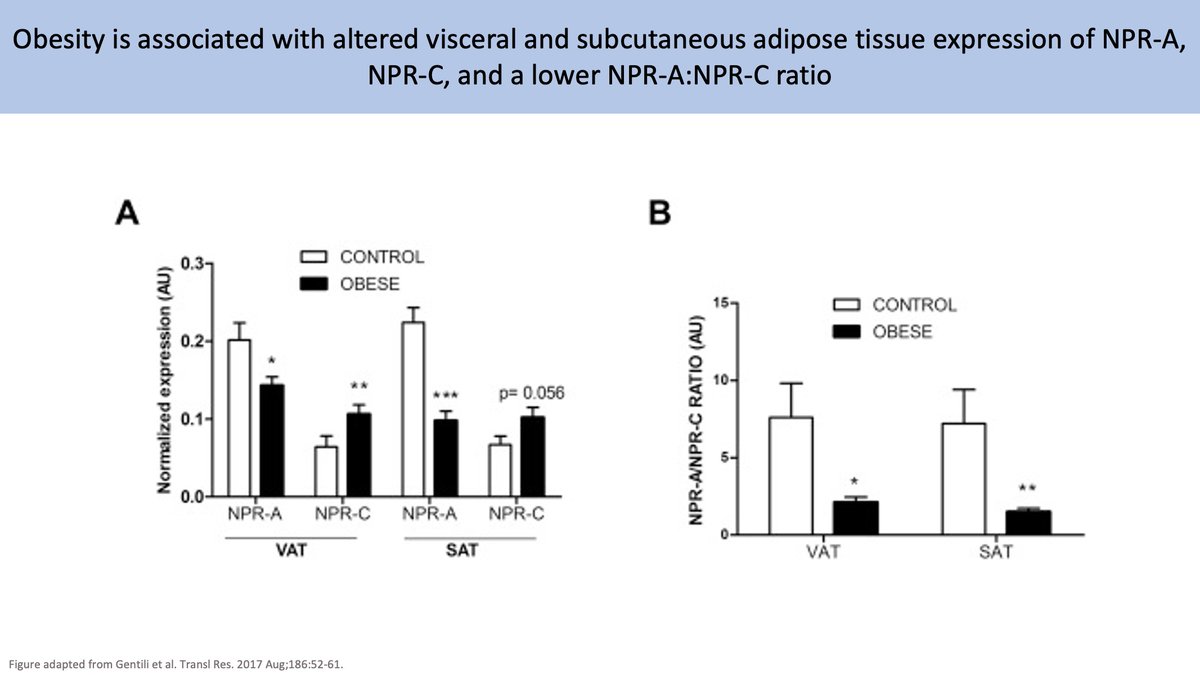
10/
1️⃣ NPR-C
Initial hypotheses focused on the disproportionate expression of NPR-C which is abundant in adipose tissue. Obesity and insulin resistance are correlated with a ⬇️ NPR-A:NPR-C ratio which may ⬆️ BNP clearance and ⬇️ BNP action.
pubmed.ncbi.nlm.nih.gov/28651075/ 🔒
1️⃣ NPR-C
Initial hypotheses focused on the disproportionate expression of NPR-C which is abundant in adipose tissue. Obesity and insulin resistance are correlated with a ⬇️ NPR-A:NPR-C ratio which may ⬆️ BNP clearance and ⬇️ BNP action.
pubmed.ncbi.nlm.nih.gov/28651075/ 🔒
11/
There is a problem with this theory: While ⬆️ NPR-C can affect BNP clearance, it doesn't explain the proportionate ⬇️ in NT-proBNP levels seen in obesity. NT-proBNP does not bind NPR-C, meaning that ⬆️ NPR-C likely does not tell the full story.
pubmed.ncbi.nlm.nih.gov/16203929/
There is a problem with this theory: While ⬆️ NPR-C can affect BNP clearance, it doesn't explain the proportionate ⬇️ in NT-proBNP levels seen in obesity. NT-proBNP does not bind NPR-C, meaning that ⬆️ NPR-C likely does not tell the full story.
pubmed.ncbi.nlm.nih.gov/16203929/

12/
This brings us to another mechanism: 2️⃣ Renal filtration.
Obesity is associated with renal hyperfiltration and ⬆️ GFR. Since BNP is freely filtered by the kidney, a relative ⬆️ in renal filtration would result in ⬆️ BNP clearance.
pubmed.ncbi.nlm.nih.gov/18234955/
This brings us to another mechanism: 2️⃣ Renal filtration.
Obesity is associated with renal hyperfiltration and ⬆️ GFR. Since BNP is freely filtered by the kidney, a relative ⬆️ in renal filtration would result in ⬆️ BNP clearance.
pubmed.ncbi.nlm.nih.gov/18234955/
13/
Finally we have 3️⃣ Neprilysin.
Interestingly, Neprilysin levels ⬆️ proportionately with BMI, likely due to ⬆️ neprilysin levels in adipose tissue. Like NPR-C, however, neprilysin does not clear NT-proBNP and likely doesn't tell the full story.
pubmed.ncbi.nlm.nih.gov/21042321/
Finally we have 3️⃣ Neprilysin.
Interestingly, Neprilysin levels ⬆️ proportionately with BMI, likely due to ⬆️ neprilysin levels in adipose tissue. Like NPR-C, however, neprilysin does not clear NT-proBNP and likely doesn't tell the full story.
pubmed.ncbi.nlm.nih.gov/21042321/

14/
So obesity does affect all 3 BNP clearance mechanisms, but perhaps we've been asking the wrong question.
Maybe the question is not "Does obesity cause low BNP?" but rather "Does low BNP cause obesity?"
It turns out that it may. Enter the "bidirectional theory of BNP".
So obesity does affect all 3 BNP clearance mechanisms, but perhaps we've been asking the wrong question.
Maybe the question is not "Does obesity cause low BNP?" but rather "Does low BNP cause obesity?"
It turns out that it may. Enter the "bidirectional theory of BNP".
15/
As we saw in the figure in tweet 3, one mechanism of BNP is to induce lipolysis.
In fact, ⬆️ BNP levels may explain the cardiac cachexia of advanced heart failure, leading some to posit that a relative lack of BNP production may contribute to obesity itself.
As we saw in the figure in tweet 3, one mechanism of BNP is to induce lipolysis.
In fact, ⬆️ BNP levels may explain the cardiac cachexia of advanced heart failure, leading some to posit that a relative lack of BNP production may contribute to obesity itself.
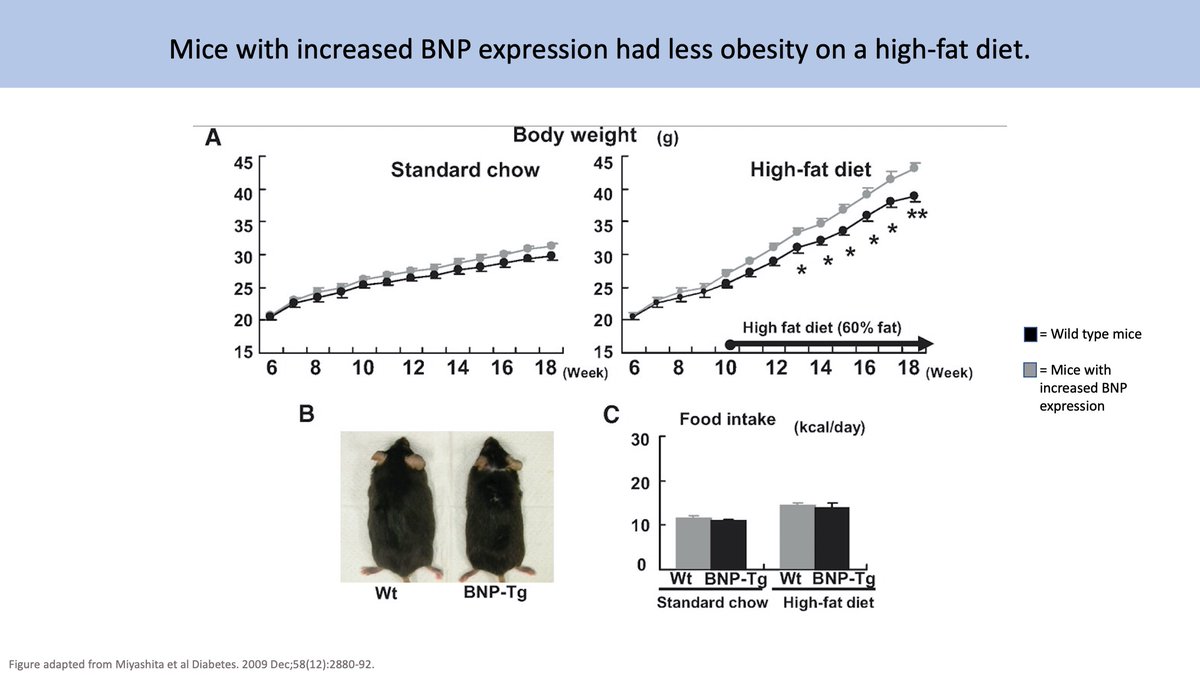
16/
This is supported by a study of BNP transgenic mice which found that ⬆️ BNP levels led to ⬆️ mitochondrial metabolic activity & size while ⬇️ BNP levels led to more obesity.
This theory merits its own tweetorial, but we'll leave this here for now.
pubmed.ncbi.nlm.nih.gov/19690065/
This is supported by a study of BNP transgenic mice which found that ⬆️ BNP levels led to ⬆️ mitochondrial metabolic activity & size while ⬇️ BNP levels led to more obesity.
This theory merits its own tweetorial, but we'll leave this here for now.
pubmed.ncbi.nlm.nih.gov/19690065/
17/
To close, let's summarize:
💥 BNP indirectly correlates with BMI
💥 Lower BNP thresholds may be needed for HF diagnosis in obesity.
💥 Obesity affects all 3 BNP clearance mechanisms: NPR-C, renal filtration, and neprilysin
💥 Low BNP levels may worsen obesity
To close, let's summarize:
💥 BNP indirectly correlates with BMI
💥 Lower BNP thresholds may be needed for HF diagnosis in obesity.
💥 Obesity affects all 3 BNP clearance mechanisms: NPR-C, renal filtration, and neprilysin
💥 Low BNP levels may worsen obesity
A huge thank you to my friend and colleague @SatyaPatelMD for his review and feedback for this tweetorial.
Also a shout-out to my former senior resident @ZacNephron who taught me this concept on my very first day of intern year.
You should follow both of them.
Also a shout-out to my former senior resident @ZacNephron who taught me this concept on my very first day of intern year.
You should follow both of them.
Lastly, in the spirit of #FOAMed I have tried to cite as many open-access sources as possible. Articles that are behind a firewall are designated with a 🔒. All others are 🆓.
Two great reviews on this specific topic:
pubmed.ncbi.nlm.nih.gov/25156856/
cardiovascmed.ch/article/doi/cv…
Two great reviews on this specific topic:
pubmed.ncbi.nlm.nih.gov/25156856/
cardiovascmed.ch/article/doi/cv…
• • •
Missing some Tweet in this thread? You can try to
force a refresh