
#HFpEF pearl of the day: In HFpEF pts with #CardioMEMS devices, bike stress echo + continuous CardioMEMS PA pressure recording can help evaluate underlying pathophysiologic abnormalities.
Case: 71 yo woman w/apical HCM, AF s/p ablation, pacemaker, HTN, CKD with cardiorenal syndrome and PH-HFpEF presents with worsening overload. Echo shows preserved LVEF with apical HCM, PASP 85 mmHg, RAP 15 mmHg, RVOT PW notching consistent with ⬆️PVR.


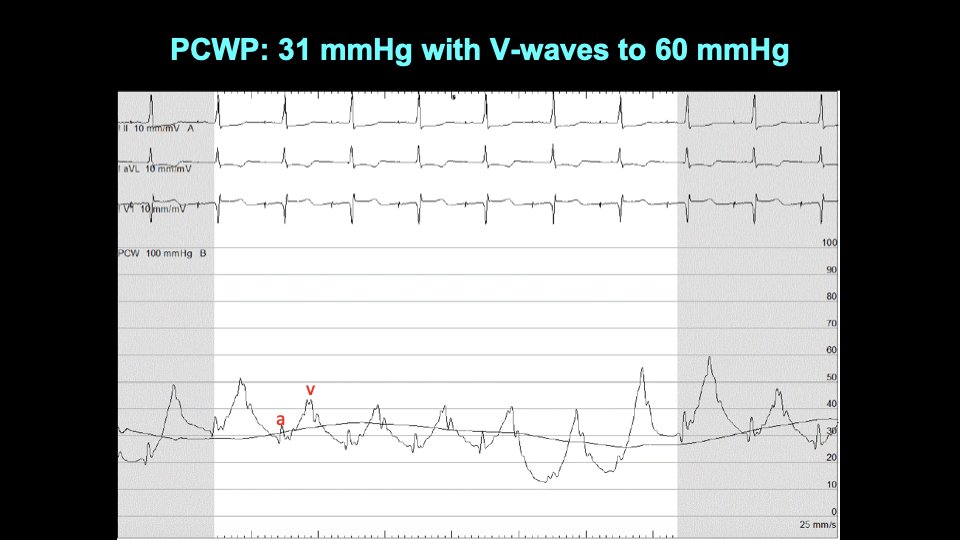
Invasive hemodynamics showed RA pressure 25 mmHg, PA pressure 92/31 (mean 54), PCWP 31 mmHg with V waves up to 60 mmHg. 

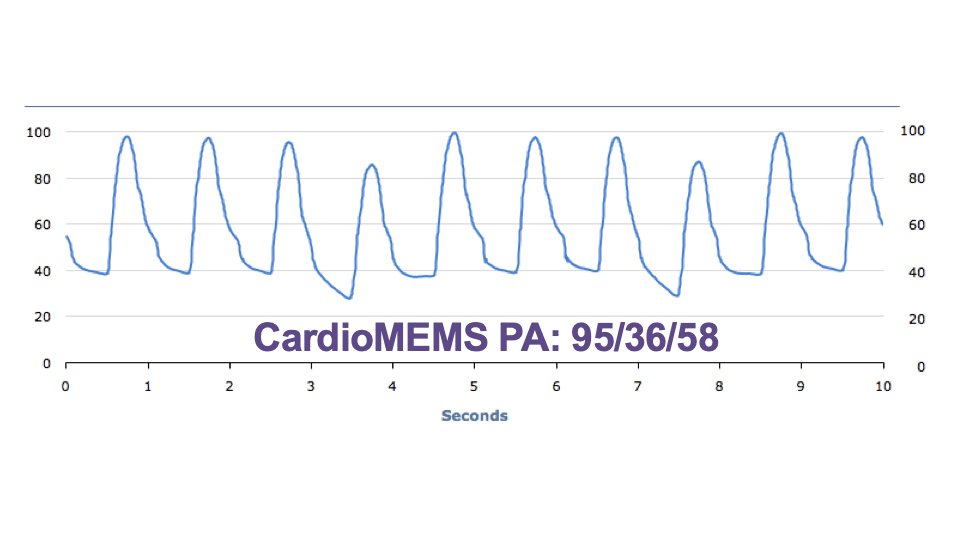
CardioMEMS placed showing good agreement with invasive hemodynamics:
She was admitted and underwent IV diuresis. Still very dyspneic. Exercise echo with continuous CardioMEMS pressure recordings done while inpatient. She could only exercise on bike to 15W. ⬆️PA pulse pressure, minimal HR increase.

Here are the CardioMEMS tracings captured during the bike stress echo:

Mitral inflow E velocity went down with exercise, suggesting underfilling of the LA:

LVOT VTI did not augment with exercise suggesting fixed stroke volume.

She had a wrist watch arterial tonometry device as well:

Systemic pulse pressure went down with exercise:

At 15W exercise, PA pulse pressure went up, and RV free wall strain got worse.

Meanwhile, at 15W exercise, LV longitudinal strain got better (augmented).

Based on the bike stress echo + CardioMEMS it seemed that SV fixed and inadequate HR, so CO was impaired. Blood trapped in the pulmonary circulation w/⬆️ PA pulse pressure and underfilling of LA/LV. Rx'd by ⬆️ basal HR on pacemaker, ⬆️ rate responsiveness: improved symptoms.
Ideally we could’ve done something to ⬆️pulmonary blood flow during exercise so that she could better ⬆️SV but unfortunately no options available. We continued to diurese and Rx her w/hemodynamic-guided mgmt but unfortunately she died ~1 yr later due to progressive renal failure.
• • •
Missing some Tweet in this thread? You can try to
force a refresh











