
More on #vaccines e.g. the full report on the Moderna vaccine which is likely to be authorized this week! By the way, there was a ? asked about vials of the Pfizer vaccine being fuller than one dose. FDA says "At this point, it is acceptable to use every full dose obtainable"
So, if each pack is 5 doses with 5 vials but you can get a 6th or 7th dose out of a vial because they are highly filled, do it, says FDA (could mean we could have 40% more doses than we thought although company may cut back from overfilling).
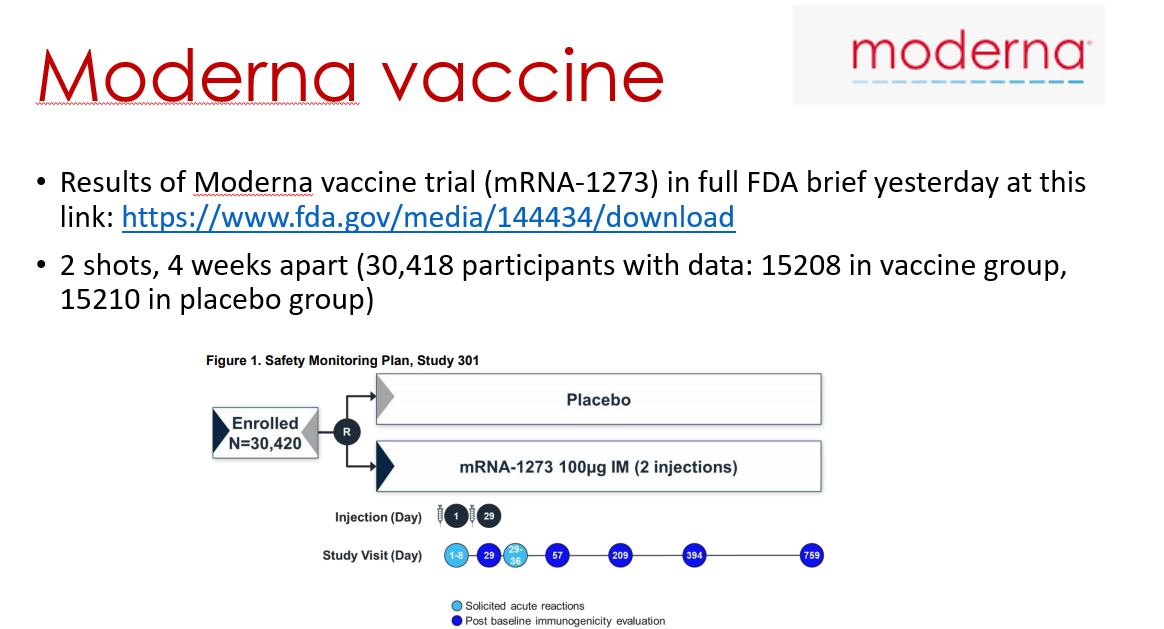
In terms of #Moderna vaccine, the full FDA brief was released yesterday and the meeting is tomorrow. Brief is here. fda.gov/media/144434/d…. I put the data into these few slides which I will now upload as pictures. 




In summary, same type of vaccine as Pfizer vaccine which is mRNA-based (surrounded by lipid layer); same efficacy 94.1%; same general safety profile (more injection sites reactions than you usually get with flu vaccine- can take Tylenol after); can be stored at less cold temps
• • •
Missing some Tweet in this thread? You can try to
force a refresh


