The U.S. has been the epicenter of the pandemic since March 26, since two weeks after COVID-19 was declared a pandemic by the WHO on March 11. This is due to failed federal response, but not all because of that but because of structure of this country, which fractures responses
and decisions to counties/states/local levels. Everyone had different responses but we are all connected so one response affects another. Also, we failed to protect workers &poor so when openings occurred or even during shutdown, people of course had to work to survive
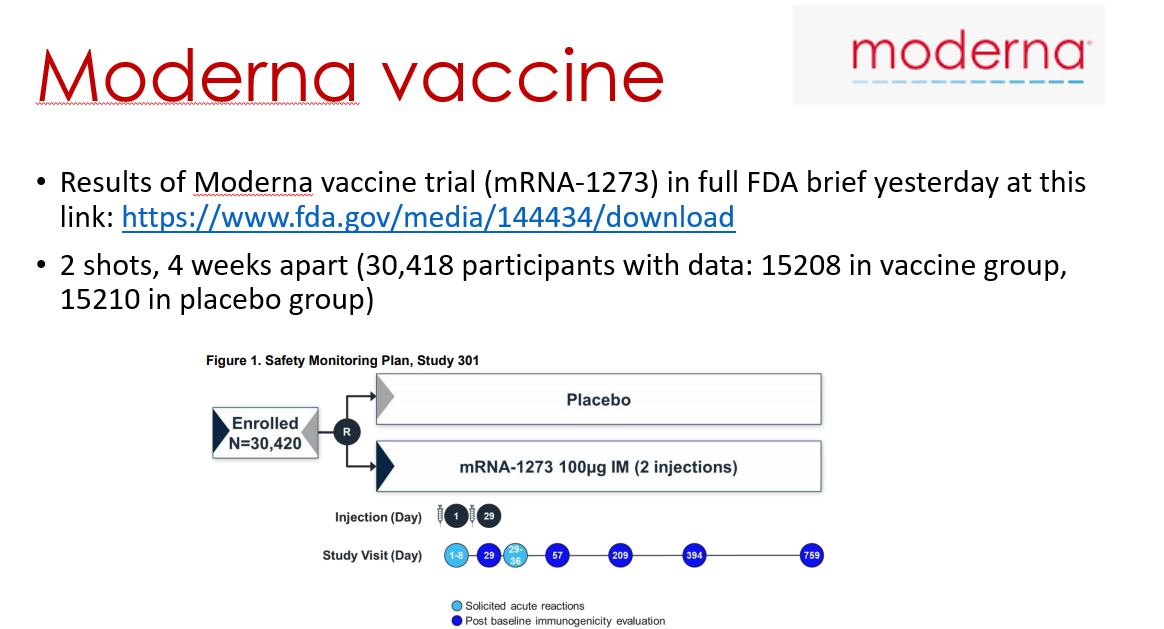
These weaknesses of our system will hopefully be strengths when it comes to vaccine distribution as that is the only way to get out of this now and local/state/counties distributing will hopefully be effective. Remember, #Moderna vaccine had 36.5% representation from communities
of color so that may help communities decide that this vaccine was really studied in a diverse group and help acceptability (Pfizer 18.1% communities of color). Here are some slides on history of #COVID & vaccines - hopeful distribution will be equitable as poor affect rich here










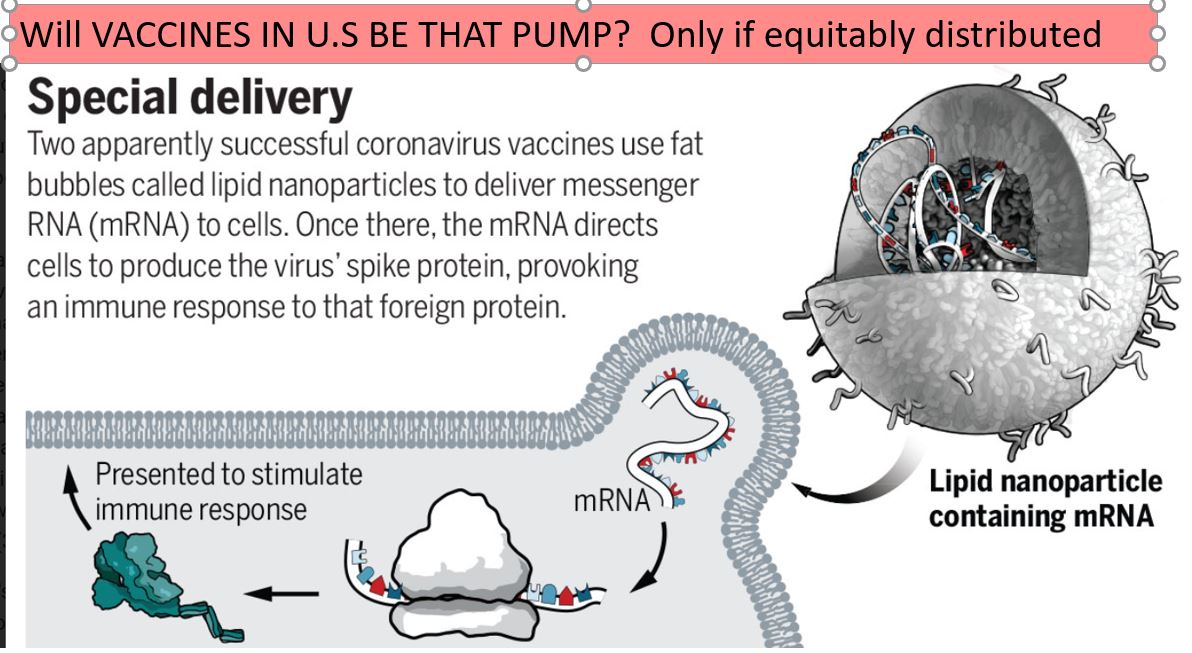
Covid-19 is devastating communities of color. Can vaccines counter racial inequity?
washingtonpost.com/health/2020/12…
washingtonpost.com/health/2020/12…





• • •
Missing some Tweet in this thread? You can try to
force a refresh