I have been told a few times that I am biased against current restrictions and it is affecting my ability to see all sides of the debate.
I appreciate being challenged to evaluate my reasoning, and I appreciate the people who do this.
I agree I am biased. Here is why. (1/x)
I appreciate being challenged to evaluate my reasoning, and I appreciate the people who do this.
I agree I am biased. Here is why. (1/x)
https://twitter.com/DavidAb10822584/status/1340395450302685197
I believe in the need for evidence-based practices.
I also believe that policies such as business closures or restrictions on life should be held to a very high standard of evidence, given all the harms that they do.
In the beginning, we did not know enough. Not anymore. (2/x)
I also believe that policies such as business closures or restrictions on life should be held to a very high standard of evidence, given all the harms that they do.
In the beginning, we did not know enough. Not anymore. (2/x)
Imagine knowing in March that after months of restrictions in CA and very lax rules in FL, this is what we would see.
Can you imagine anyone saying back then "Yeah, we should lockdown hard"?
Not a single person would support business closures. (3/x)
Can you imagine anyone saying back then "Yeah, we should lockdown hard"?
Not a single person would support business closures. (3/x)


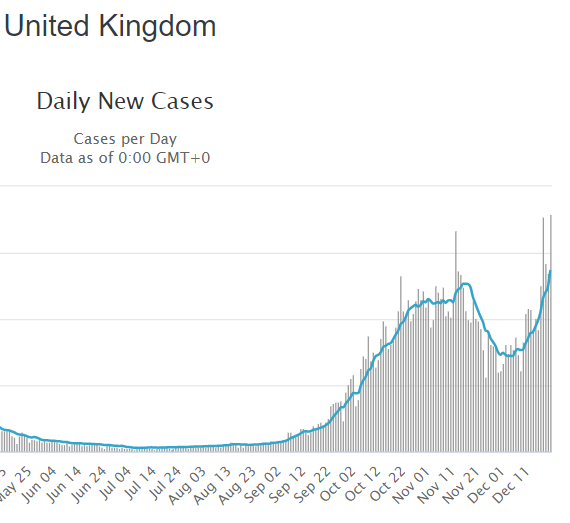
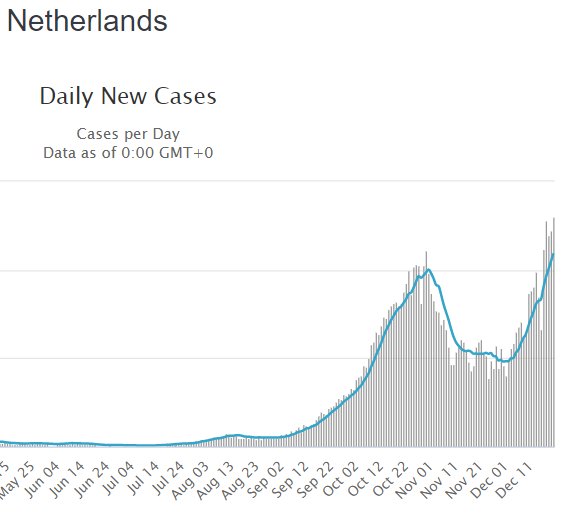
Real world evidence keeps showing that with or without government touch, curves go down when it is time.
Remember the doom Sweden was about to face, and then how it became "They are doing worse than their neighbors?"
I do. (4/x)
Remember the doom Sweden was about to face, and then how it became "They are doing worse than their neighbors?"
I do. (4/x)
https://twitter.com/covidtweets/status/1340291094827986947?s=20
I believe reasons why people support lockdowns have not been rational for a long time. They are psychological.
Sunk cost fallacy. Fear. Tribalization. Illusion of control. Consistency bias. Internal locus of control.
These are why we still have people supportive of them. (5/x)
Sunk cost fallacy. Fear. Tribalization. Illusion of control. Consistency bias. Internal locus of control.
These are why we still have people supportive of them. (5/x)
Lockdowns have not affected my life much, except for having to change how I teach a little. My income keeps coming. I was not much of a social butterfly before either.
Yet these restrictions, done haphazardly without any evidence, outrage me as I watch lives crumbling. (6/x)
Yet these restrictions, done haphazardly without any evidence, outrage me as I watch lives crumbling. (6/x)
Seeing how people act selfishly and with entitlement, and then package it as "caring for others" outrage me.
Seeing kids being sacrificed despite being at essentially zero risk outrage me.
Seeing people say they follow the science and then stay blind to data outrage me. (7/x)
Seeing kids being sacrificed despite being at essentially zero risk outrage me.
Seeing people say they follow the science and then stay blind to data outrage me. (7/x)
So yeah, I am a bit biased.
Forgive me. Or don't.
I will continue to be biased. (8/8)
Forgive me. Or don't.
I will continue to be biased. (8/8)
• • •
Missing some Tweet in this thread? You can try to
force a refresh