I'm rather concerned by the inability of Test-and-Trace to explain the diagnostic accuracy of the lateral flow test. This was the statement about the performance of Innova in the School Handbook sent out by Test-and-Trace before Xmas. 

"As accurate in identifying as PCR" is simply not true. Specificity tells you about false positives, not true positives. It tells you the proportion of those without COVID who correctly get negative results. It doesn't tell you how could the test is at identifying cases.
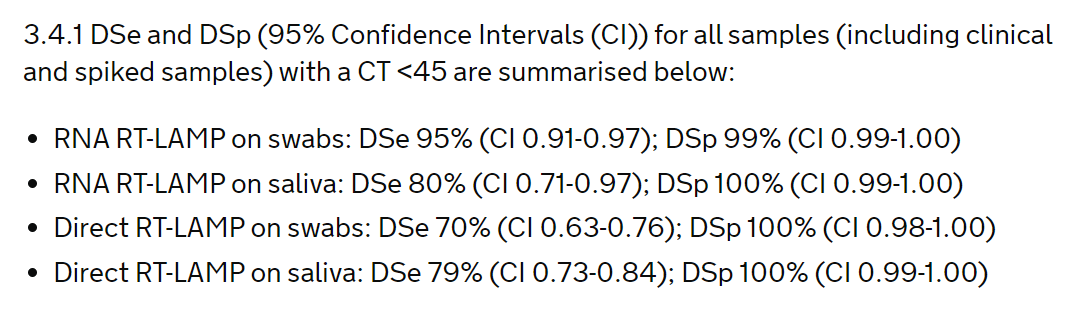
And interesting that the high figure for specificity is stated, but no numbers for sensitivity are given (which are much lower - 40% in Liverpool). We don't want selective reporting from our Health Department.
Now I'm pleased the document has been updated, but I am not that impressed that it is replaced with:

An improvement, but the phrase "very accurate" is ambiguous and likely to imply to many that this is a good test. And nothing here actually tells you how well the test works. Its the sort of marketing type explanation you see from manufacturers, but what we want from the DHSC
This does not provide a "fully informed basis" for schools to decide what to do, or how to discuss the test with their pupils. If this were a clinical trial this would fail the ethics committees approval for the patient information sheet.
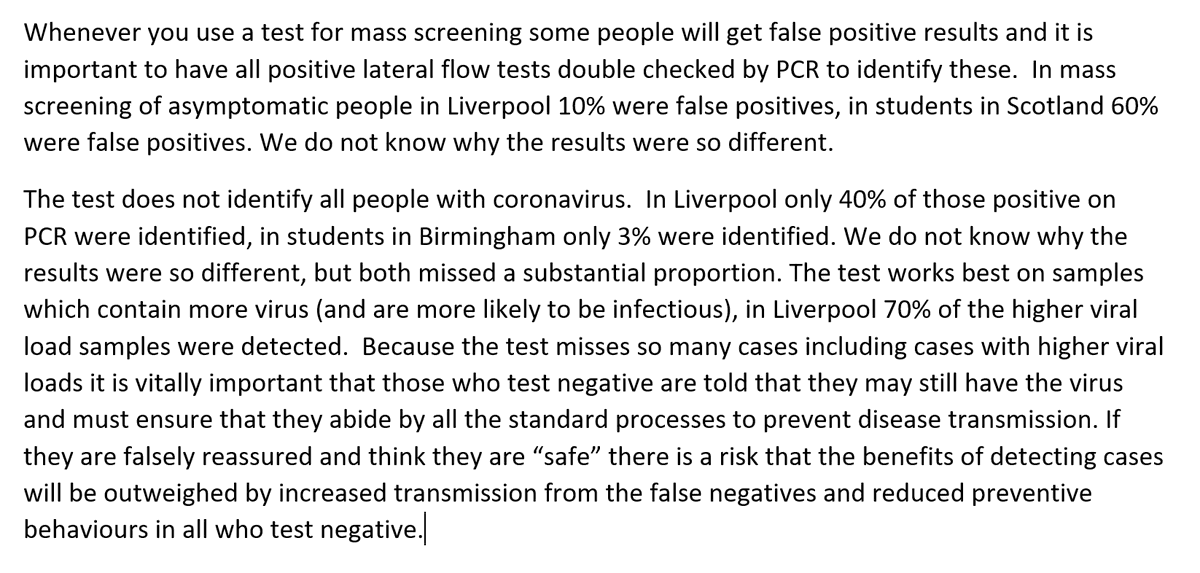
My suggested replacement is rather more words but hopefully more informative.
• • •
Missing some Tweet in this thread? You can try to
force a refresh