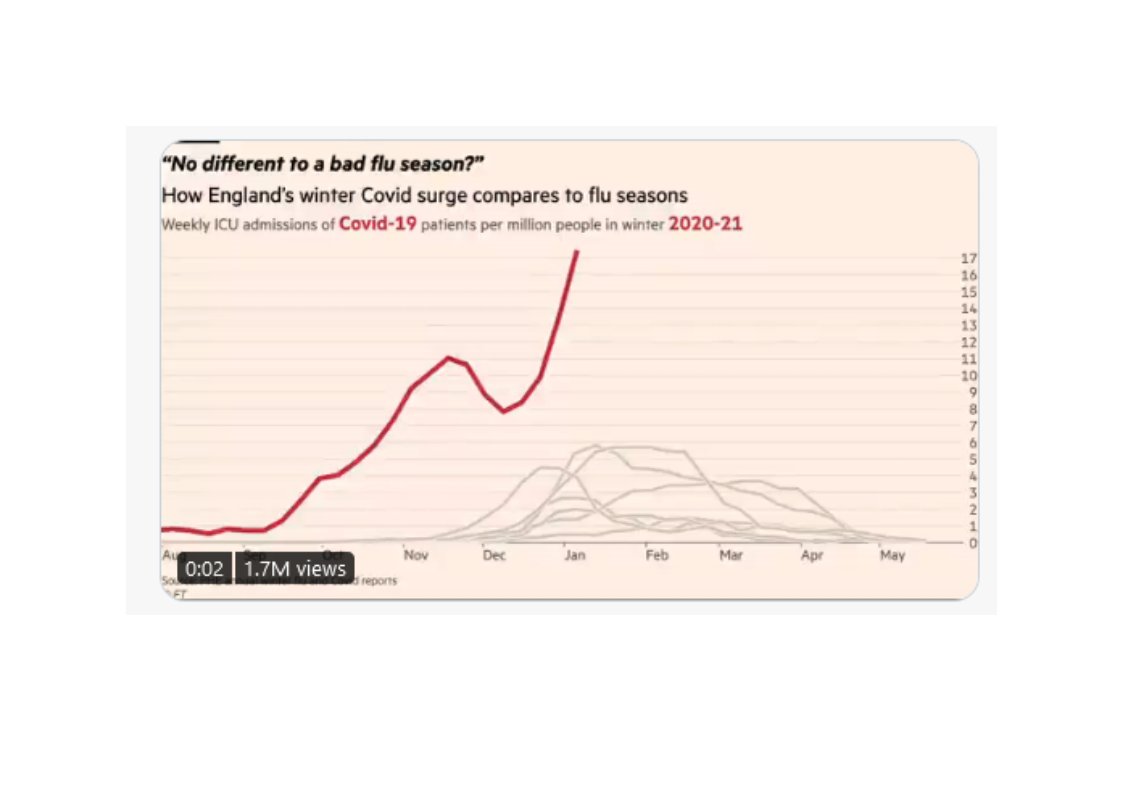
26/42 Are there any national datasets that accurately capture what is going on? The brilliant @jburnmurdoch has highlighted number of admissions into ICU. The message from his animated chart (click on link) couldn’t be clearer – this winter is v unusual: 
https://twitter.com/i/status/1347200811303055364.
27/42 Some sceptics arguing covid-19 tests are inaccurate. PCR tests not 100% accurate but hospital inpatient testing accuracy much increased by frequency of testing (typically admission, days 3 & 6/7, then weekly). This means very low numbers of overall false positives.
28/42 Some sceptics argue that the published covid-19 positive inpatient numbers include both those admitted with covid-19 and those who acquired covid-19 in hospital. And that there are significant numbers of patients who have acquired covid-19 in hospital.
29/42 Covid-19 positive test data has always included anyone testing positive, irrespective of initial diagnosis. And the NHS has always acknowledged that hospital acquired (nosocomial) infection is a big issue. Hospitals are working incredibly hard to control it….
30/42 …The NHS regularly and completely transparently publishes nosocomial infection data, by hospital. But neither issue affects the degree of pressure that hospitals are under. Every inpatient, irrespective of initial diagnosis/infection source, occupies a hospital bed.
31/42 Some sceptics using regular @ONS & @PHE_uk mortality data to argue that current death rates are just reflecting ordinary mortality rates for this time of year. Or that the covid-19 mortality definition and diagnoses are mixing up ordinary respiratory illness and covid-19.
32/42 This excellent thread
https://twitter.com/Mike_aka_Logiqx/status/1347912835595186177looks at these issues in detail. It shows clearly why it is too early for the current sets of this data to be showing increased levels of mortality from the current, new variant driven, surge of covid-19 infection.
33/42 In the words of this thread: “If you are using the ONS + PHE data to assess excess deaths that are happening *now* you are using the wrong data because of lags. The impact of this surge will only become apparent in future data from the ONS + PHE”.
34/42 The current covid-19 death definition widely accepted across medical profession. Doctors are required by law to complete death certificate to the best of their knowledge and ability. Covid deaths are running at an alarming rate – currently over 1,000 a day.
35/42 Some sceptics are arguing that the failure to use Nightingales before now indicates that the NHS isn’t that busy. They are not purpose built hospitals and would require staff to be transferred from other settings. Systematic use was always a last resort insurance policy…
36/42 …The NHS was always going to use every ounce of permanent purpose built capacity first. The fact that the London Nightingale is opening next week is a sign of how pressured the NHS in London has become. Other Nightingales – e.g. Exeter and Manchester – already in use.
37/42 Particularly loathsome are the videos of empty corridors and hospital areas. There are lots of good reasons why some areas of hospitals will be much quieter than usual. No visitors due to infection control. Outpatient clinics moved online. Films being done at night-time…
38/42 …Waiting areas not in use due to social distancing. Reduced levels of ordinary planned surgery. Most activity and staff in hospitals will currently will be concentrated on covid, intensive care and emergency areas. Areas where illegal filmers can’t film.
39/42 And, as this thread from @dpjhodges -
https://twitter.com/DPJHodges/status/1347555844884410378- argues. If the sceptics are right, those charged with nation’s health – CMO, CSA, Ministers, officials, NHS leaders – all have to be unaware of the data problems sceptics have "identified"...
40/42 …And despite their decades of cumulative experience, they are making major public health decisions totally oblivious to the catastrophic misreading of the data that the amateur lock-down sceptic sleuths have uncovered…
41/42 ...or they are unaware of these catastrophic misreadings. And, for reasons no one has yet rationally explained, they are all carrying on regardless, day after day, month after month, perpetuating one of the greatest public health hoaxes in history.
42/42 Worth adding that the more evidence & data driven sceptics now abandoning sceptical camp: spectator.co.uk/article/lockdo…. Still time for rest to follow! Particularly since everyone in NHS from frontline staff and trust leaders to @NHSEngland CEO is heartily fed up of this cr*p.
• • •
Missing some Tweet in this thread? You can try to
force a refresh