We shouldn’t be too fixated on vaccine efficacy. What ultimately is important (& I suspect most of us are talking about) is vaccine effectiveness (VE).
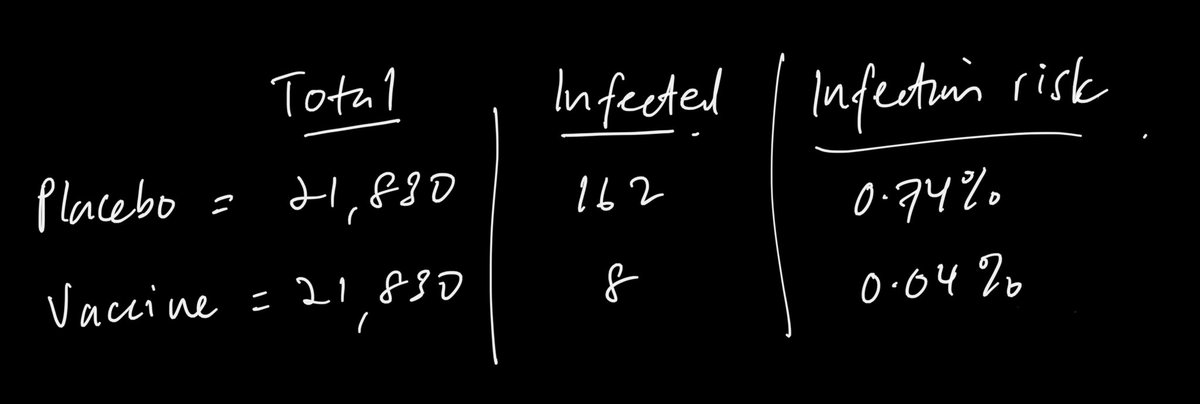
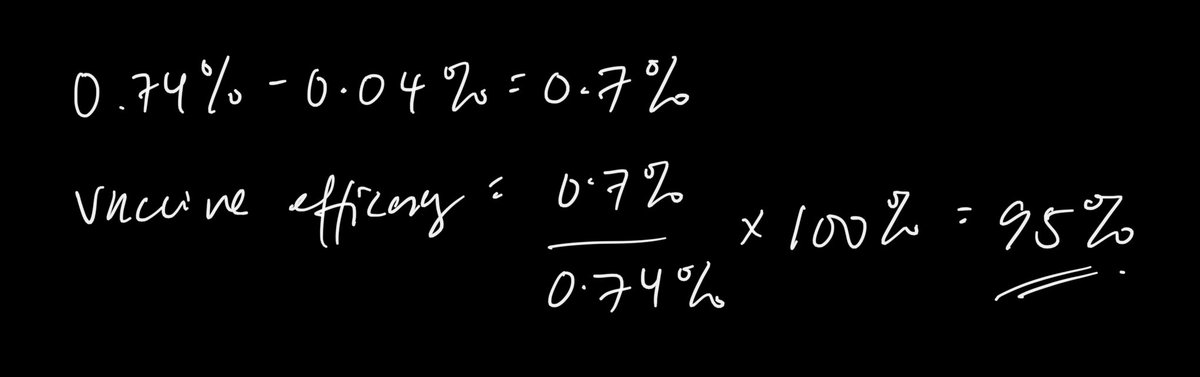
Vaccine efficacy is % of reduction of disease in a vaccinated vs unvaccinated group in a trial.
VE is the real world impact.
Vaccine efficacy is % of reduction of disease in a vaccinated vs unvaccinated group in a trial.
VE is the real world impact.
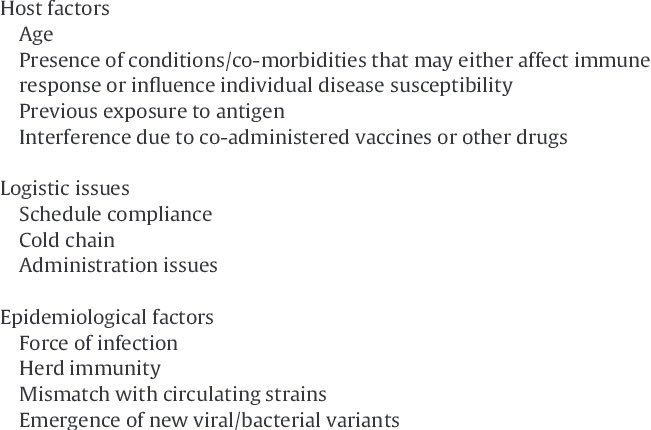
V.efficacy measures individual protection in a controlled environment while VE looks at how protected is a population after vaccination. There is a whole host of factors influencing it.
And not necessarily v.efficacy is directly proportional to VE.
And not necessarily v.efficacy is directly proportional to VE.
Focusing on only efficacy will distract us from implementing a good vaccination plan to maximise effectiveness.
Factors like administration, cold chain, coverage (which impacts herd immunity) all can greatly increase effectiveness, which is what we want.
Factors like administration, cold chain, coverage (which impacts herd immunity) all can greatly increase effectiveness, which is what we want.
Ideally yes, we would want a 100% efficacy vaccine and translate it to 100% effectiveness. But that wont happen in the real world.
Vaccinating 70% or more of the population with a 50% efficacy vaccine is better than vaccinating 30% of the population with a 90% efficacy vaccine.
Vaccinating 70% or more of the population with a 50% efficacy vaccine is better than vaccinating 30% of the population with a 90% efficacy vaccine.
Most of us are looking at the vaccine through a transmission lens. We want it to be ‘effective’ so we can go back to our pre-Covid lives; travel, socialise, etc.
But so far the vaccines r not designed for that. The primary endpoint is to decrease disease or death. Which it does.
But so far the vaccines r not designed for that. The primary endpoint is to decrease disease or death. Which it does.
Data from trials shows it can reduce disease burden, therefore reduce hospital overloading & reduce complications/death. This is a big win.
The messaging should be clear. It is not for us to travel, socialise without the usual SOPs.
The messaging should be clear. It is not for us to travel, socialise without the usual SOPs.
But I suppose the market is ‘spoiled’ by the Pfizer, Moderna etc with their >90% numbers. I call it the Asian mother effect.
Vaccine X: I got 70%
Asian mother: 70%? Why not 90%? 100%?
😂
Vaccine X: I got 70%
Asian mother: 70%? Why not 90%? 100%?
😂
In a nutshell, we have to look at the various nuances of immunisation; efficacy, effectiveness, herd immunity (a thread for another day).
My opinion remains,
Vaccinate wide, vaccinate fast, vaccinate safe. #VaccineStrategy
My opinion remains,
Vaccinate wide, vaccinate fast, vaccinate safe. #VaccineStrategy
• • •
Missing some Tweet in this thread? You can try to
force a refresh