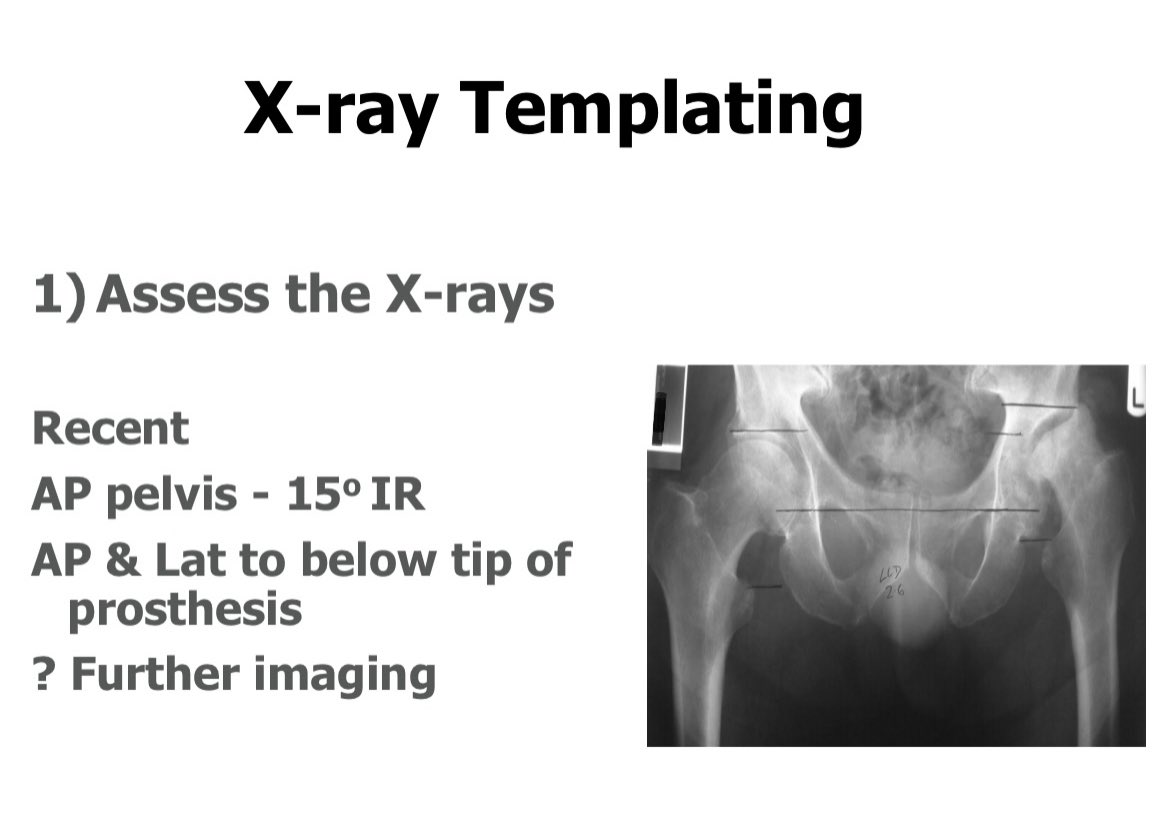
52/365 good radiographs are key, now for a systematic approach to assessment
https://twitter.com/exeterhipunit/status/1350549387454394368
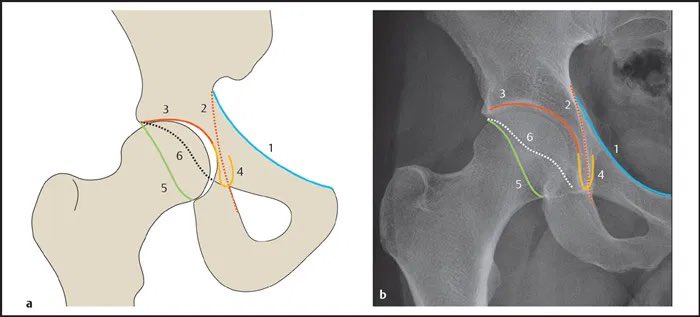
Firstly, some acetabular radiographer anatomy
1 iliopubic line - the ant column
2 ilioischial line - the post column
3 the acetabular fossa
4 the teardrop - medial inferior socket
5 post wall
6 ant wall
1 iliopubic line - the ant column
2 ilioischial line - the post column
3 the acetabular fossa
4 the teardrop - medial inferior socket
5 post wall
6 ant wall
Assess the bone deficiency or excess. Where is it? If a deficient acetabulum: is it contained (intact front, back, medial, superior walls) or uncontained. This should feed into the type of reconstruction, the prosthesis and the need for bone graft.

If excess bone, are these osteophytes and if so, where are they. These can be helpful landmarks intraoperatively but can make assessment of anatomy a challenge. Are they going to affect your approach, can you remove easily? Is there HO? Do you need to consider Rx?

Draw two lines. Start with a teardrop line (line A). This is your datum, your reference. If the teardrops aren’t clear use the bottom of the obturator foramen as an alternative. Then draw the roof line (line B) parallel to line A. Start on the normal side and translate to other



In this case you can there is a small supero-lat deficiency. There is femoral head above the roof line showing acetabular bone has been eroded. Therefore, in this case, expect a deficiency. So if you start teaming and there is no deficiency, there is a risk you are reaming high.
All part of planning. If you know where you’re going and how to get there, and something doesn’t look as you expect, there’s a chance you’ve gone wrong somewhere. Don’t be afraid to stop and reassess.

• • •
Missing some Tweet in this thread? You can try to
force a refresh