
SWITCH TO PREMIUM MASKS—I’ve been saying it for months. We need to switch to KN95, KF94, or European FFP2 masks ASAP. The new #b117 #COVID19 is just too contagious. Cloth isn’t enough anymore folks. Germany 🇩🇪 & Austria 🇦🇹 mandating on all public transits. washingtonpost.com/world/europe/e… 

2) there are many masks that have 94/95% filtration...
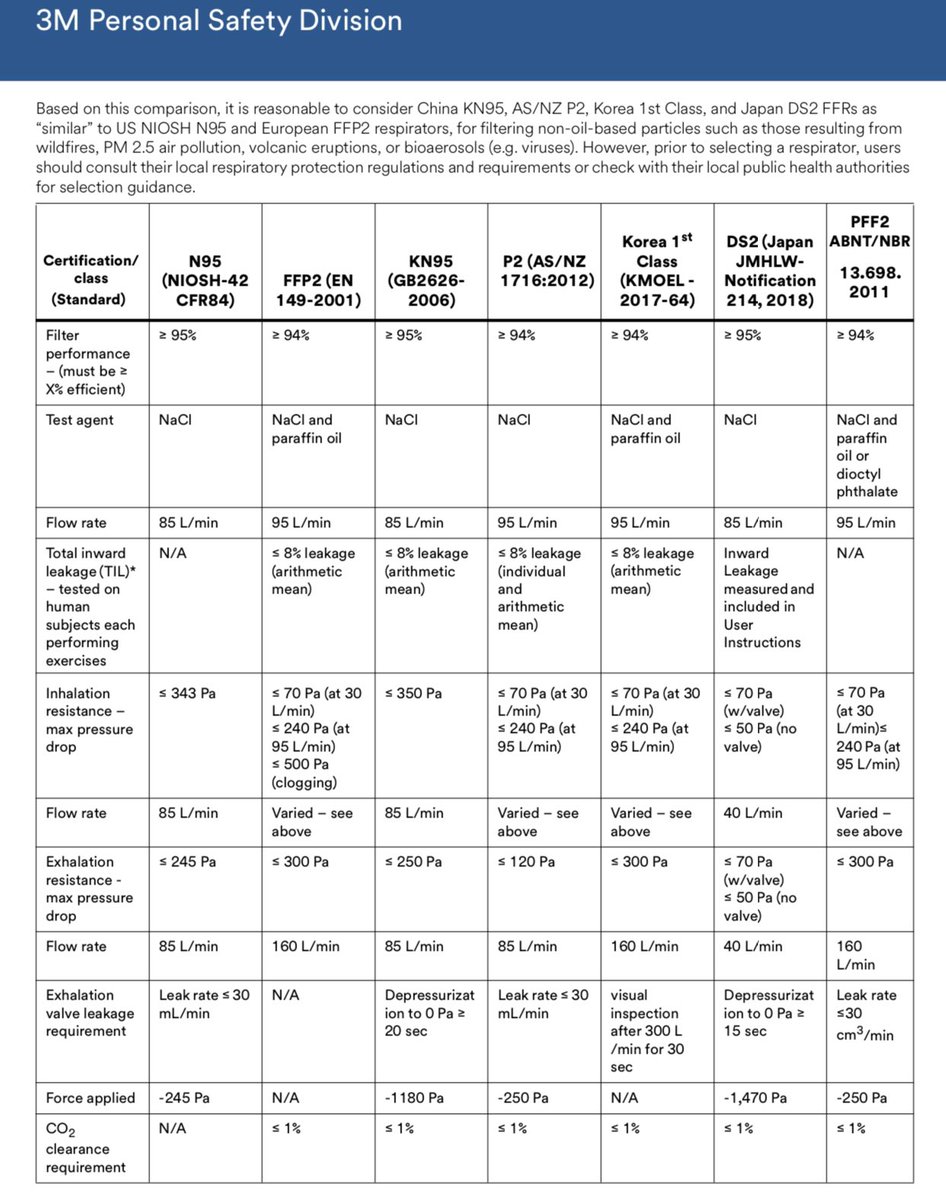
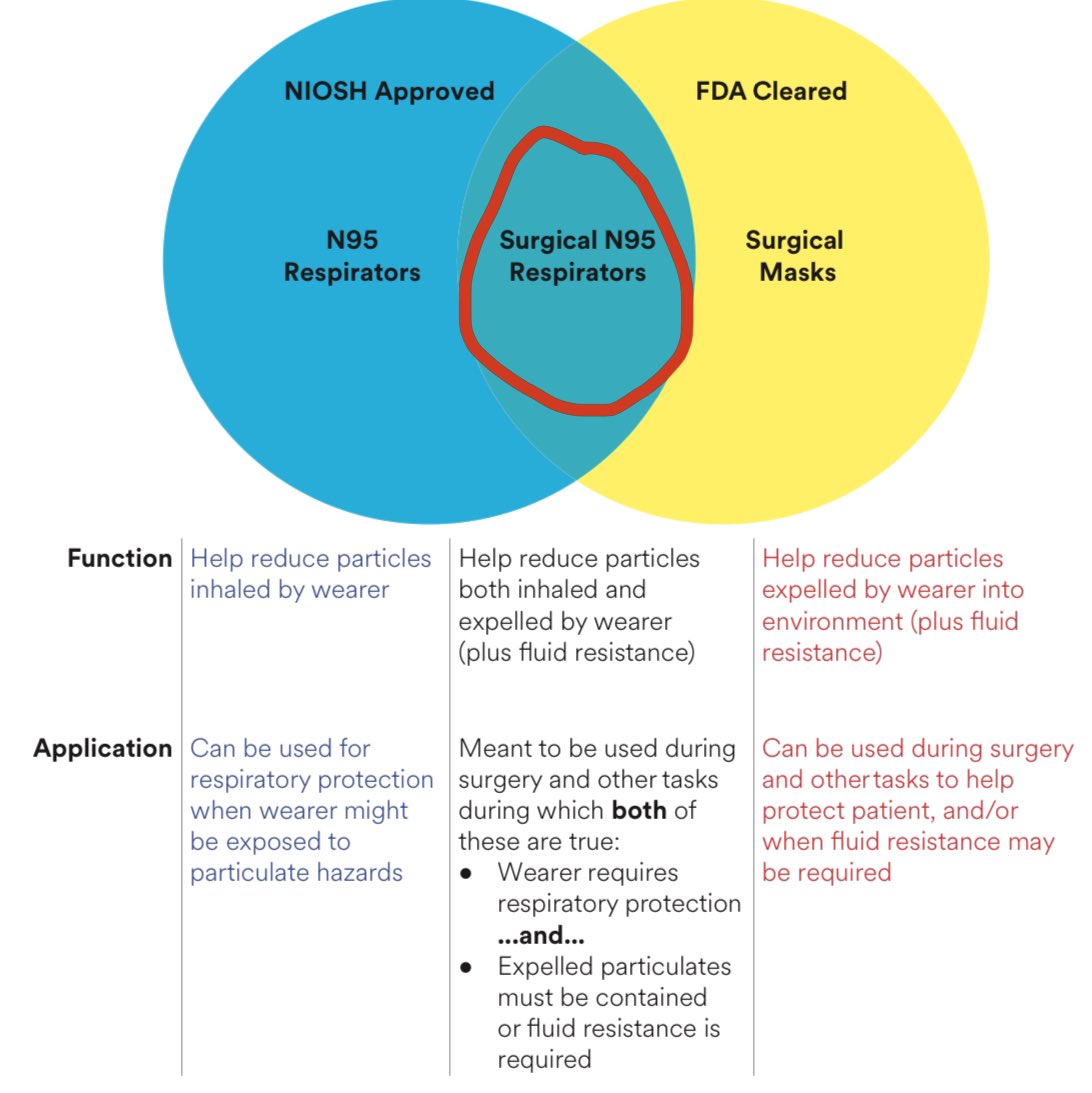
3) N95 masks are more rare outside of hospitals because they are in shortage and needed by HCWs. You might find some NIOSH N95 from wood working, but note those are often not fluid resistant.

4) Like Germany and Austria, in France, the country’s health advisory council on Monday discouraged the wearing of inefficient cloth and homemade masks, also arguing they may not offer sufficient protection against the more highly transmissible coronavirus variants.
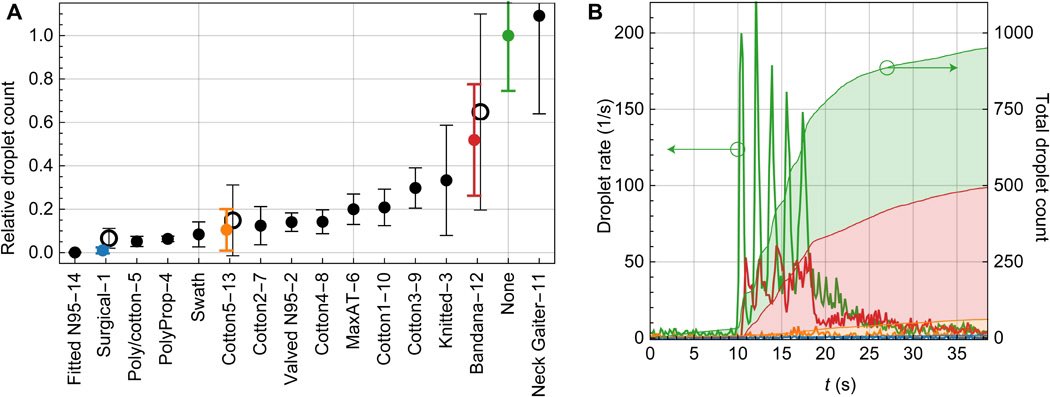
5) of all the masks tested, N95 grade and surgical masks were superior this mask study. N95 class the best — they didn’t test KN95 but we know they are similar in filtration (but less perfect in fit tightness). But KN95 and KF94 and FFP2 all 94/95% good.
advances.sciencemag.org/content/6/36/e…
advances.sciencemag.org/content/6/36/e…
6) FFP2 masks (resemble KN95) in Europe are now $1.2 each these days ($2-3 before) after EU negotiated with manufacturers.
Also get this — low income families get these premium FFP2 masks **for free**!!!
Also get this — low income families get these premium FFP2 masks **for free**!!!
https://twitter.com/DrEricDing/status/1349001505978912770
7) Some call FFP2 masks “N95” on some boxes in EU. This was just 2 euros each. Made in U.K. 🇬🇧 as well as in Germany.
https://twitter.com/DrEricDing/status/1349005300767068163
8) My favorite premium mask is the South Korea 🇰🇷 made KF94 that everyone wears there. It has a folding system that leaves more space for your mouth — so much that you forget you’re wearing a mask when you’re speaking! You can find them online.
https://twitter.com/DrEricDing/status/1316195796908470272
9) Double masking (like Joe Biden when he traveled last year) also works. Or if you have a mask with a vent, wear another mask over the vented one.
https://twitter.com/DrEricDing/status/1316191229655363584
10) There are also kids FFP2 and KN95 masks for better fit for kids too. Masks must FIT TIGHTLY or else leakage around nose bridge makes it less effective.
GOOD FIT == mask will expand when u exhale and push inward when you inhale. If your mask doesn’t, it’s too loose.
GOOD FIT == mask will expand when u exhale and push inward when you inhale. If your mask doesn’t, it’s too loose.
11) I honestly fiddle with nose bridge of a new mask a lot sometimes when i first get a new one— I press the nose bridge tightly first and then stick it on my nose to shape it. Pre press it then put on nose to shape it most efficiently. If you glasses fog up—there is a leak.
12) There are fake N95 / KN95 being sold right now. Just be careful. I can’t say which are real or fake but they do exist.
Staples and many major stores now sell KN95s. Presumably (?) they sell legit ones. I also directly order KF94 from S Korea & FFP2 from relatives in Europe.
Staples and many major stores now sell KN95s. Presumably (?) they sell legit ones. I also directly order KF94 from S Korea & FFP2 from relatives in Europe.
https://twitter.com/DrEricDing/status/1257376598615040000
14) To be clear, cloth masks do work too, just to lesser degree. And cloth is to catch your droplets more rather than be good inhalation filters. That’s why cloth works best when >95% of people wear them. But if many anti mask, then that is less effective.
14b) This was last week—they now mandating the premium masks in more places in Europe now. As result they are being given out free or subsidized to just $1.20 each in stores in Europe. We need Biden WH to DPA produce them here soon.
https://twitter.com/DrEricDing/status/1349000463035854852
15) For more on the science of masks and an good detailed evidence thread, see this earlier 🧵 below.
https://twitter.com/DrEricDing/status/1309829079152111616
16) Why do I care so much?
1 year ago today, I posted the “HOLY MOTHER OF GOD” warning to the world.
Hope it helped some folks keep their families safe. Please be careful everyone.
nymag.com/intelligencer/…
1 year ago today, I posted the “HOLY MOTHER OF GOD” warning to the world.
Hope it helped some folks keep their families safe. Please be careful everyone.
nymag.com/intelligencer/…

17) Why am I so concerned about #B117? Because many many models all show it will likely take over countries in infect and we lose buffer of what little containment we do half if it takes over.
https://twitter.com/DrEricDing/status/1346899021621813249
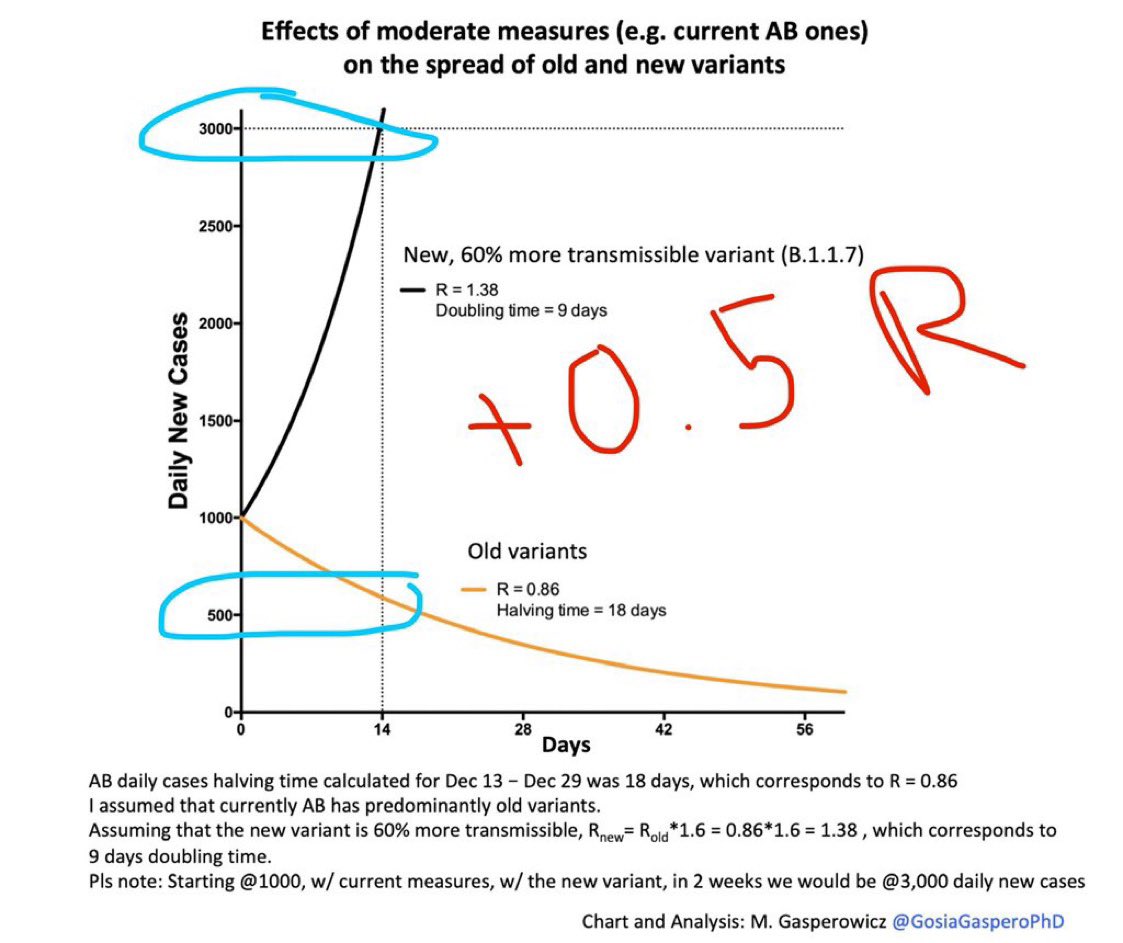
18) Notably, the #B117 variant virus is such a beast—suppose we have 1000 cases/day now... with an R=0.86 we could reduce it to 500/day in 2 weeks.
➡️But w/ added contagiousness of B117 variant that has ~60% higher R, in 2 weeks, 3000 new cases/day instead—
6x vs old ⚠️
➡️But w/ added contagiousness of B117 variant that has ~60% higher R, in 2 weeks, 3000 new cases/day instead—
6x vs old ⚠️
19) UK 🇬🇧 former health minister now also urging mandates for premium masks on mass transit and shops. news.sky.com/story/covid-19…
20) What is the best source of premium masks? That would be @projectn95. Their masks are the most thoroughly vetted as authentic. And they are a nonprofit organization.
https://twitter.com/projectn95/status/1353839562011922434
21) @projectn95 also fulfills N95 grade masks for both public and healthcare providers. Their email is listed below.
I receive zero commissions and not been paid in any way for this post.
@projectn95 is simply one of the best nonprofits.
projectn95.org/ppe-for-public
I receive zero commissions and not been paid in any way for this post.
@projectn95 is simply one of the best nonprofits.
projectn95.org/ppe-for-public
22) A reckoning of all the ways the Trump WH failed on PPE procurement and lack of sufficient mask production.
nytimes.com/2020/11/17/mag…
nytimes.com/2020/11/17/mag…
• • •
Missing some Tweet in this thread? You can try to
force a refresh




















