Following on from the first dose Pfizer data below where 7/15 participants above the age of 80 did not achieve neutralisation of virus, we report that all 15 have achieved neutralisation 3 weeks after second dose.
https://twitter.com/GuptaR_lab/status/1350131626240598019
It could be that >80 yo are slower in mounting responses but this is unlikely and also leaves people vulnerable despite vaccine. Remember >80 y o are not featuring in trials so they might still get severe disease. Pre print to come but significant delays.
We should add that the second dose was given at 3 weeks after the first. Likely we should stick to this schedule in those above 80 years. Huge effort from @damicollier @rpdatir @CambridgeBRC
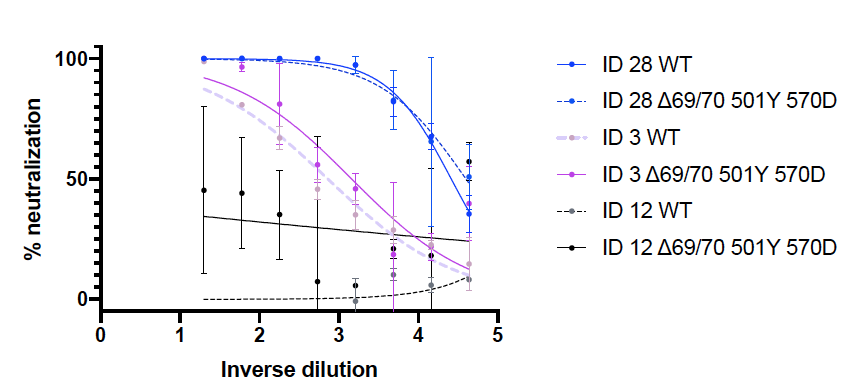
Here are the neutralisation curves after first and second doses for six of the poor responders in the >80 age group. We show how much we can suppress a virus using the antibodies from vaccines. The flat lines show a poor effect after first dose but great improvement after second 

Should also say that I am firmly supportive of plans to extend dosing to 12 weeks in order to achieve better control of transmission, just that we might need to consider subgroups differently in order to get the best out of our vaccine supplies.
• • •
Missing some Tweet in this thread? You can try to
force a refresh