
#Tweetorial1️
✅Only ~40-60% of GEA pts receive 2L Rx in the USA, & the treatment landscape is fragmented.
📌 pubmed.ncbi.nlm.nih.gov/25792290/
📌pubmed.ncbi.nlm.nih.gov/31056940/
@TumorBoardTues #TumorBoardTuesday
✅Only ~40-60% of GEA pts receive 2L Rx in the USA, & the treatment landscape is fragmented.
📌 pubmed.ncbi.nlm.nih.gov/25792290/
📌pubmed.ncbi.nlm.nih.gov/31056940/
@TumorBoardTues #TumorBoardTuesday

#Tweetorial2
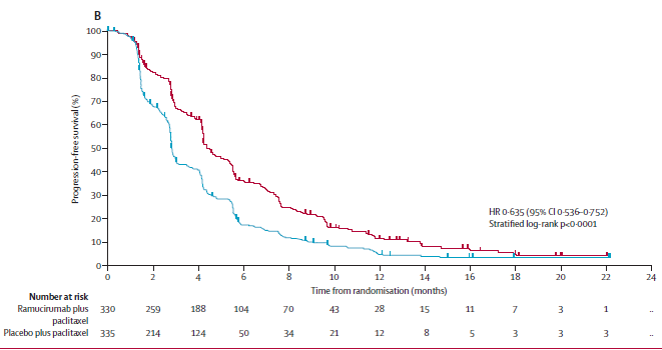
✅The Phase III 2L RAINBOW study of paclitaxel-Ram vs Paclitaxel had improved OS, serving as a benchmark SOC
📌thelancet.com/journals/lanon…
✅The Phase III 2L RAINBOW study of paclitaxel-Ram vs Paclitaxel had improved OS, serving as a benchmark SOC
📌thelancet.com/journals/lanon…

#Tweetorial3
✅The Phase III 2L KN061 study showed detriment for pts with PDL1 CPS 0 treated w pembro vs paclitaxel (no Ram!), and terminated this group early.
(green = pembro, red = paclitaxel)
📌 thelancet.com/journals/lance…
📌 thelancet.com/journals/lance…
✅The Phase III 2L KN061 study showed detriment for pts with PDL1 CPS 0 treated w pembro vs paclitaxel (no Ram!), and terminated this group early.
(green = pembro, red = paclitaxel)
📌 thelancet.com/journals/lance…
📌 thelancet.com/journals/lance…

#Tweetorial4
✅Studies show that FOLFIRI is an option vs paclitaxel, along w ramucirumab, in certain situations-
1) persistent oxaliplatin neuropathy or
2) previous Rx with platinum/taxane perioperatively or 1L:
📌 pubmed.ncbi.nlm.nih.gov/30470690/
📌 ascopubs.org/doi/abs/10.120…
✅Studies show that FOLFIRI is an option vs paclitaxel, along w ramucirumab, in certain situations-
1) persistent oxaliplatin neuropathy or
2) previous Rx with platinum/taxane perioperatively or 1L:
📌 pubmed.ncbi.nlm.nih.gov/30470690/
📌 ascopubs.org/doi/abs/10.120…


#Tweetorial5a
✅2L studies were -ve for anti-HER2 Rx in 2L:
📌 Phase 3 TyTAN (lapatinib) pubmed.ncbi.nlm.nih.gov/24868024/
📌 Phase 3 GATSBY (TDM1) pubmed.ncbi.nlm.nih.gov/28343975/
📌 Phase 2 T-ACT (trastuzumab) pubmed.ncbi.nlm.nih.gov/32208960/
✅2L studies were -ve for anti-HER2 Rx in 2L:
📌 Phase 3 TyTAN (lapatinib) pubmed.ncbi.nlm.nih.gov/24868024/
📌 Phase 3 GATSBY (TDM1) pubmed.ncbi.nlm.nih.gov/28343975/
📌 Phase 2 T-ACT (trastuzumab) pubmed.ncbi.nlm.nih.gov/32208960/
#Tweetorial5b
Some contributing reasons for these -ve studies include:
1) Allowed HER2 IHC0/1+ w FISH+ (based on pre-1L profile) (TyTAN = (35%!))
2) Not rechecking HER2 status after PD on 1L Rx (all 3 studies)
✅ A subgroup of T-ACT tumors at just prior to 2L 69% (!) were HER2-
Some contributing reasons for these -ve studies include:
1) Allowed HER2 IHC0/1+ w FISH+ (based on pre-1L profile) (TyTAN = (35%!))
2) Not rechecking HER2 status after PD on 1L Rx (all 3 studies)
✅ A subgroup of T-ACT tumors at just prior to 2L 69% (!) were HER2-
#Tweetorial5c
3) Relatively small studies w ⬇️ power
✅ Despite this, in TyTAN, ORR ITT was 27% vs 9% in favor of pac/lap vs pac,
✅ & in those with pre-1L IHC3+ (who r less likely to evolve to neg @ 2L) --> OS advantage (ORR not reported but likely higher: 40%?, 50%?):
3) Relatively small studies w ⬇️ power
✅ Despite this, in TyTAN, ORR ITT was 27% vs 9% in favor of pac/lap vs pac,
✅ & in those with pre-1L IHC3+ (who r less likely to evolve to neg @ 2L) --> OS advantage (ORR not reported but likely higher: 40%?, 50%?):


#Tweetorial6️
✅Recent papers evaluating HER2 conversion show rates of conversion between 15-45%.
✅ The longer the pt is on & over more lines of anti-HER2 Rx may increase this finding.
📌 pubmed.ncbi.nlm.nih.gov/29122777/
📌 pubmed.ncbi.nlm.nih.gov/33234578/
✅Recent papers evaluating HER2 conversion show rates of conversion between 15-45%.
✅ The longer the pt is on & over more lines of anti-HER2 Rx may increase this finding.
📌 pubmed.ncbi.nlm.nih.gov/29122777/
📌 pubmed.ncbi.nlm.nih.gov/33234578/

#Tweetorial7
✅Tras-Derux in Asian phase 2 in 3L+ (~55% 3L, 45% 4L+) showed better ORR, PFS, and OS compared to MD choicetaxane/irinotecan.
📌 nejm.org/doi/full/10.10…
📌Approved in Japan for 3L+ 9/25/20
📌Approved by FDA for 2L+ 🤔 1/15/21.
Black Box: ILD, Reassess HER2 bx!
✅Tras-Derux in Asian phase 2 in 3L+ (~55% 3L, 45% 4L+) showed better ORR, PFS, and OS compared to MD choicetaxane/irinotecan.
📌 nejm.org/doi/full/10.10…
📌Approved in Japan for 3L+ 9/25/20
📌Approved by FDA for 2L+ 🤔 1/15/21.
Black Box: ILD, Reassess HER2 bx!




CASE DISCUSSION
👇👇👇
👇👇👇

#Tweetorial8a Case Discussion 1/2
✅ CPS 0 (no pembro), per #KN061
✅ ctDNA HER2 -ve (despite PT HER2+) predicts likely failure here systemically. I would use Chemo+Ram as their next best 2L option.
(Welcome comments on this point - let's debate! 😎)
✅ CPS 0 (no pembro), per #KN061
✅ ctDNA HER2 -ve (despite PT HER2+) predicts likely failure here systemically. I would use Chemo+Ram as their next best 2L option.
(Welcome comments on this point - let's debate! 😎)
#Tweetorial8b Case Discussion 2/2
✅ tumor biopsies can be useful for reassessing tumor biology:
📌 pubmed.ncbi.nlm.nih.gov/33234578/
✅ but so can liquid biopsies be useful for reassessing tumor biology, and may better represent the dz in its entirety:
📌 pubmed.ncbi.nlm.nih.gov/31427281/
✅ tumor biopsies can be useful for reassessing tumor biology:
📌 pubmed.ncbi.nlm.nih.gov/33234578/
✅ but so can liquid biopsies be useful for reassessing tumor biology, and may better represent the dz in its entirety:
📌 pubmed.ncbi.nlm.nih.gov/31427281/


#Tweetorial9a
✅ For persistently HER2+ tumors, phase 3 2L studies are ongoing, both requiring retesting to confirm HER2+:
📌 Pac/Ram vs Pac/Ram/Tucatinib/Trastuzumab clinicaltrials.gov/ct2/show/NCT04…
📌 Pac/Ram vs T-DXd clinicaltrials.gov/ct2/show/NCT04…
✅ For persistently HER2+ tumors, phase 3 2L studies are ongoing, both requiring retesting to confirm HER2+:
📌 Pac/Ram vs Pac/Ram/Tucatinib/Trastuzumab clinicaltrials.gov/ct2/show/NCT04…
📌 Pac/Ram vs T-DXd clinicaltrials.gov/ct2/show/NCT04…
#Tweetorial9b
*My Opinion: With 10% ILD risk, moving T’Dxd earlier than 3L should require direct large-scale comparison to standard Pac/Ram and most importantly, to other SOC (readily available) as well as investigational anti-HER2 approaches. 🧐
Cheers 🍻and Happy Valentine's💝
*My Opinion: With 10% ILD risk, moving T’Dxd earlier than 3L should require direct large-scale comparison to standard Pac/Ram and most importantly, to other SOC (readily available) as well as investigational anti-HER2 approaches. 🧐
Cheers 🍻and Happy Valentine's💝
And for me this is the preferred regimen for all patients second line
SUMMARY:
#targetedtherapiesfortargetedpopulations
Treating with the right drug, at the right dose, at the right time. 😎 #MedTwitter #TumorBoardTuesday
#targetedtherapiesfortargetedpopulations
Treating with the right drug, at the right dose, at the right time. 😎 #MedTwitter #TumorBoardTuesday
• • •
Missing some Tweet in this thread? You can try to
force a refresh









{kind=link}