I think @ChrisGiles_ is basing his point on schools on the fact that prevalence is down more amongst school age children than 70+.
But if you look at the timing of the trends, I don't think the ONS data really scream out that closing schools reduces infections.
But if you look at the timing of the trends, I don't think the ONS data really scream out that closing schools reduces infections.
https://twitter.com/ChrisGiles_/status/1360219174476406788
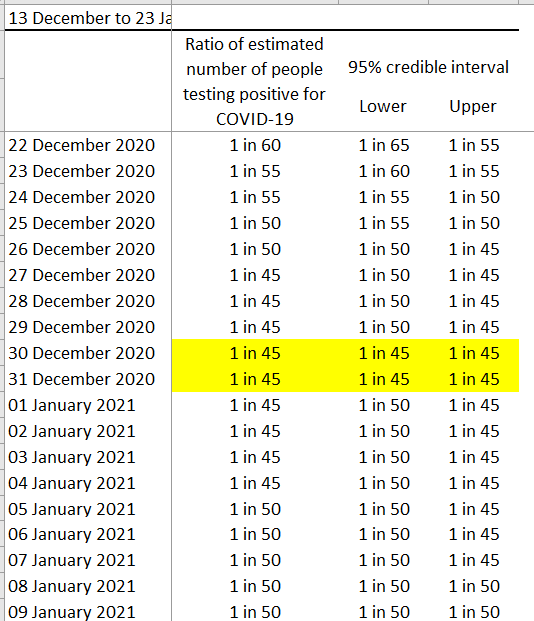
Changes in prevalence will reflect changes in infections about 2 weeks earlier. Take age 2-year 6 group (mainly primary). Estimated prevalence increased until a peak on 24 Dec (implying infections peaked about 10 Dec). So infections started falling at a time schools were open.
Prevalence falls until 6 Jan (i.e. infections about 23 Dec) & then increases again. i.e. infections in primary kids started increasing again when schools were shut for holidays.
Prevalence starts falling again from 18 Jan, i.e. infections falling from about 4 Jan, exactly when lots of primary schools kids were in school.
You might even argue the prevalence data suggests closing schools increases infections but, given possible Christmas effects & uncertainty over the incidence-prevalence lag, that would be a stretch.
As for HE moving online. In-person teaching had finished by 9 Dec, but most stopped a week or so earlier. So any effect on prevalence in yr 12-age 24 group should be evident well before Christmas. In fact ONS has peak for that group on 30 Dec.
The ONS modelled age estimates have quite wide confidence intervals so we should be cautious with using them to make inferences. But these data certainly don't seem to me to be telling us that tells us that school closure/moving HE online reduces infections.
As for hospitality, in most of the country it was shut for most of the (if not the whole) period including when infections were going up as well as down, so not sure the prevalence data really tell us that closing pubs reduces infections either.
• • •
Missing some Tweet in this thread? You can try to
force a refresh