Restrictions were imposed to stop health services being overwhelmed.
Govt policy on reopening now seems to be based on an assumption that opening 1 thing inevitably increases transmission & so something else has to be kept shut.
There is little support for this in the data ...
Govt policy on reopening now seems to be based on an assumption that opening 1 thing inevitably increases transmission & so something else has to be kept shut.
There is little support for this in the data ...
E.g. A number of academic papers suggest opening schools has little or no impact on transmission rates:
academic.oup.com/cid/advance-ar…
medrxiv.org/content/10.110…
iza.org/publications/d…
So why should pubs stay shut longer because schools are open? Or retail or gyms?
academic.oup.com/cid/advance-ar…
medrxiv.org/content/10.110…
iza.org/publications/d…
So why should pubs stay shut longer because schools are open? Or retail or gyms?
The evidence of significant transmission from outdoor sports is v. weak, even contact sports like rugby: bjsm.bmj.com/content/early/…
So why should allowing sport be conditional on anything else?
So why should allowing sport be conditional on anything else?
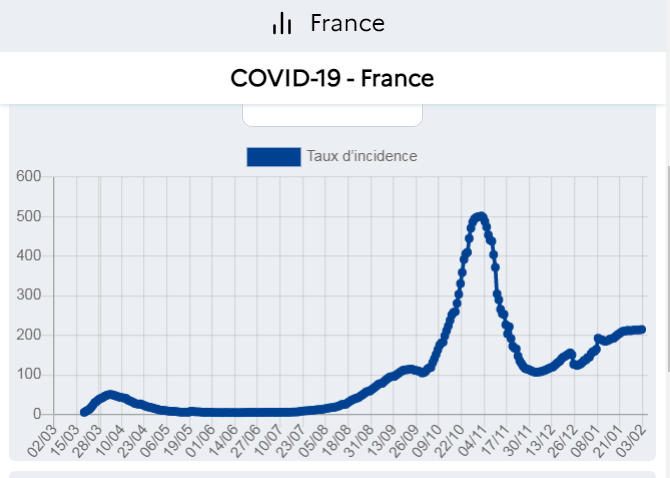
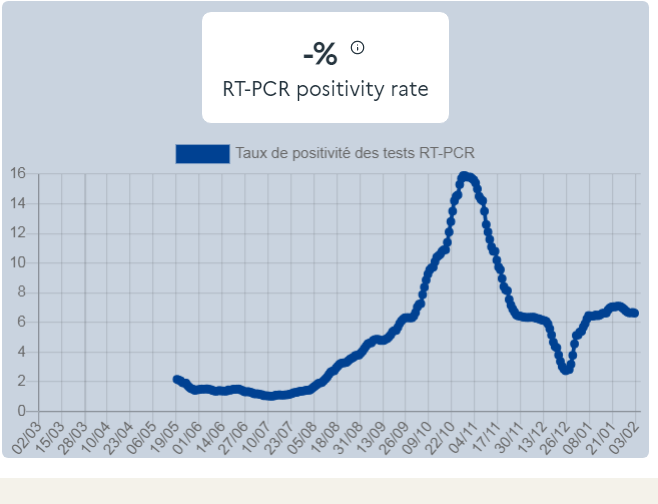
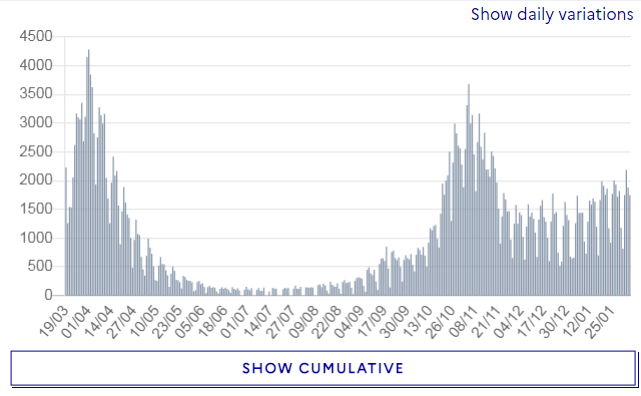
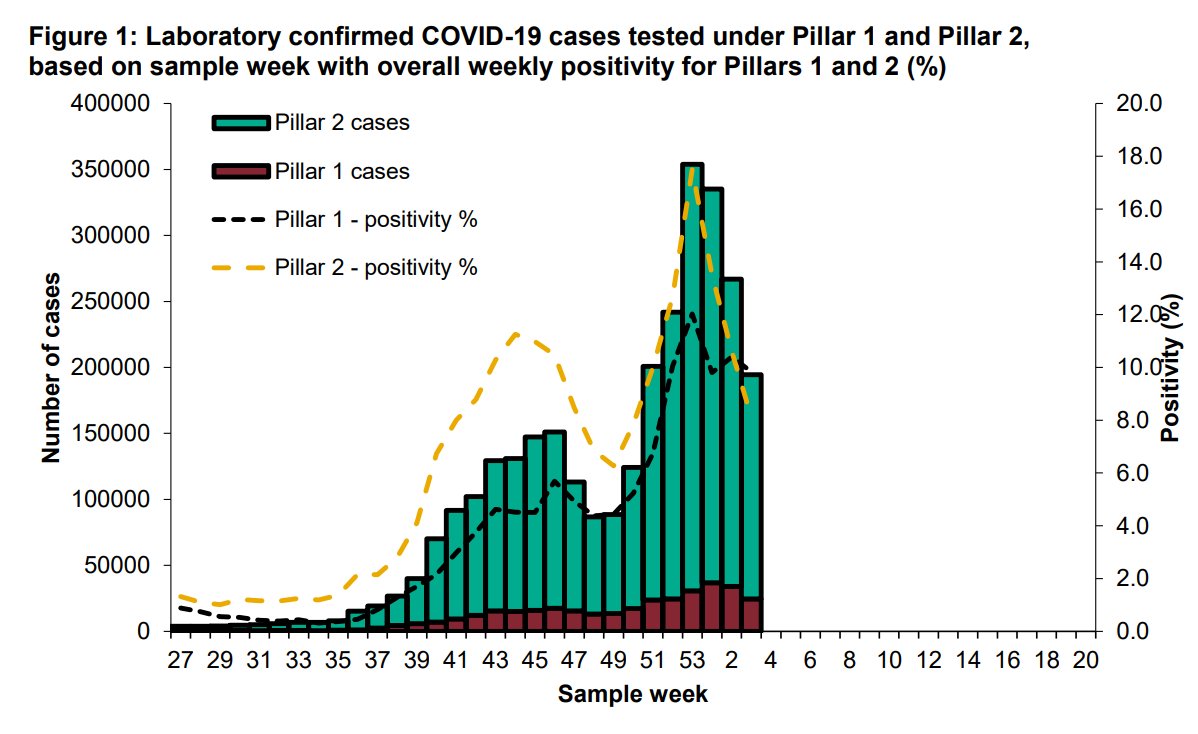
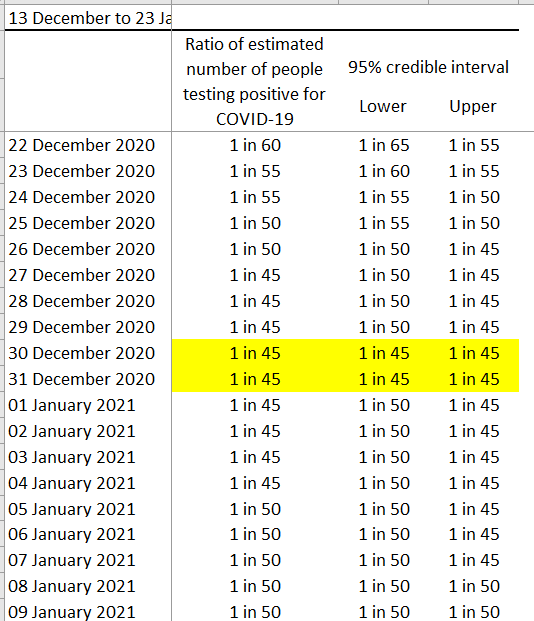
Remember also that hospital admissions are now 57% lower than their January peak January. Positive tests are 75% lower. Given the lag, admissions are set to fall even more in coming days.
Govt approach to reopening should be this:
no legal restriction or compulsory measure stays in place for even 1 more day unless there is strong evidence that
a. removing the restriction risks health services being overwhelmed
&
b. its effectiveness exceeds the costs it imposes.
no legal restriction or compulsory measure stays in place for even 1 more day unless there is strong evidence that
a. removing the restriction risks health services being overwhelmed
&
b. its effectiveness exceeds the costs it imposes.
• • •
Missing some Tweet in this thread? You can try to
force a refresh