THINK LIKE AN EPIDEMIOLOGIST: Lately I have been asked why we are seeing a dramatic turnaround in cases in the US. Is it vaccines? Herd immunity? An artifact due to a drop in testing? Behavior change? Weather?? A few tweets about how I step through this question. 1/6 

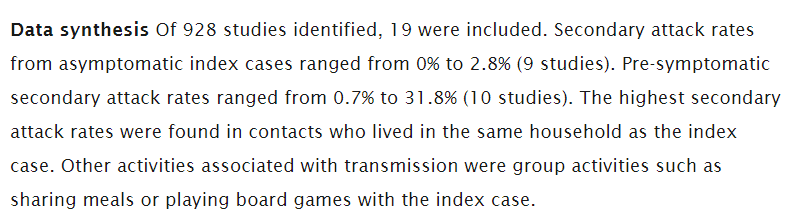
To start, I look to see whether the drop is an artifact. While testing has dropped somewhat, it's not enough to explain the rapid drop in cases. A drop in testing would also not explain the drop in hospitalizations that is consistent across regions. 2/6
covidtracking.com/data/charts
covidtracking.com/data/charts

I then consider the similarity of the drop across locations, looking by subregion and by state. The similar patterns seen are relevant because different places have different vaccination coverage, levels of acquired immunity, and weather. Why the turnaround at a similar time? 3/6


I also note the dramatic speed of the drop. Weather has not changed much over the last few weeks. Vaccination coverage is quickly increasing (and is targeted!), but we have not achieved broad coverage yet. And the turnaround started a few weeks ago. 4/6
covid.cdc.gov/covid-data-tra…
covid.cdc.gov/covid-data-tra…

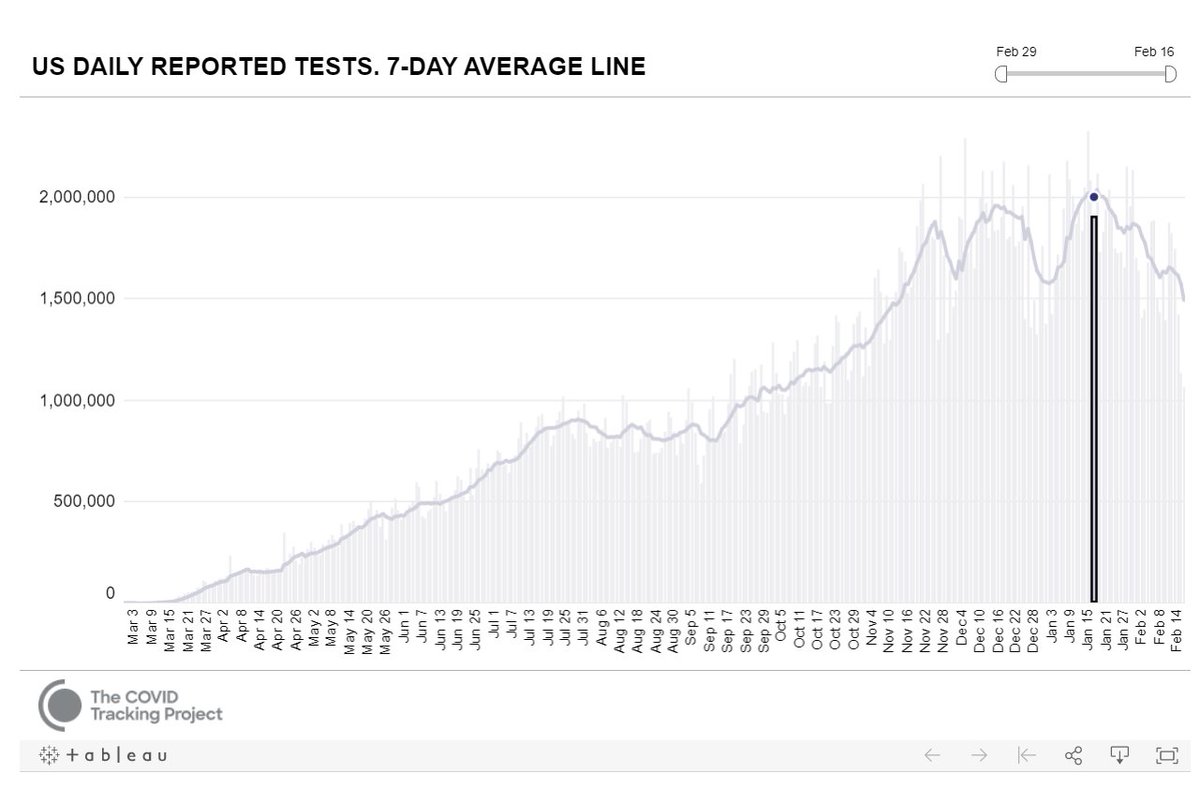
It reminds me a bit of the quick summer turnaround in Florida. The timing of the slowdown was similar across areas in Florida, which to me signaled that herd immunity was not the major driver. That plus the resurgence we have seen in FL this winter. 5/6
covid.cdc.gov/covid-data-tra…
covid.cdc.gov/covid-data-tra…
Taken together, I think the most likely explanation is a mix of policy and individual-level behavior change, as people react to what they see in the news and in their communities, but helped along by acquired immunity due to widespread infection plus targeted vaccination. 6/6
Addendum. A few folks have mentioned the holidays, which I didn't touch upon in the thread, but are relevant as they temporarily expanded our social networks. For what it's worth, the thread is just as much about the thought process as the answers. Add your own insights below!
• • •
Missing some Tweet in this thread? You can try to
force a refresh