2 Shades of Gray in Susceptibility Weighted Imaging (SWI)
A #RadInTraining #TWEETORIAL for #radiologists & #radres on technical aspects and #neurorad clinical applications of SWI, inspired by @radiology_rsna review:
pubs.rsna.org/doi/10.1148/ra…
(Figures adapted from article)
1/15
A #RadInTraining #TWEETORIAL for #radiologists & #radres on technical aspects and #neurorad clinical applications of SWI, inspired by @radiology_rsna review:
pubs.rsna.org/doi/10.1148/ra…
(Figures adapted from article)
1/15

2/ SWI can distinguish between which of the following?
3/ ANSWER: All of the above
SWI is a gradient-echo MR sequence that accentuates local magnetic field distortions from paramagnetic (i.e. hemosiderin) and diamagnetic (i.e. calcification) properties through signal loss in the form of T2*. Phase data can highlight these differences
SWI is a gradient-echo MR sequence that accentuates local magnetic field distortions from paramagnetic (i.e. hemosiderin) and diamagnetic (i.e. calcification) properties through signal loss in the form of T2*. Phase data can highlight these differences
4/ Understanding phase data in SWI is vendor dependent. In a left-handed system phase is positive going clockwise while in a right-handed system phase is positive going counter-clockwise. Signal intensity of gray matter can be used to determine handedness.

5/ Left-handed system: microbleed appears HYPOintense centrally and HYPERintense peripherally.
Right-handed system: microbleed appears HYPERintense centrally and HYPOintense peripherally.
Right-handed system: microbleed appears HYPERintense centrally and HYPOintense peripherally.

6/ Choice of imaging parameters depends on field strength and structures of interest for visualization.
➡️1.5T require longer TEs to get same susceptibility effect as 3T or 7T --> longer TR and lower signal-to-noise ratio (SNR)
➡️Spatial resolution of 0.5 x 0.5 mm3 is preferred
➡️1.5T require longer TEs to get same susceptibility effect as 3T or 7T --> longer TR and lower signal-to-noise ratio (SNR)
➡️Spatial resolution of 0.5 x 0.5 mm3 is preferred
7/ Apart from detecting microbleeds, optimizing SWI has led to multiple new clinically applicable signs:
☑️Nigrosome 1 (Swallow tail) sign in Parkinson Disease
☑️Central vessel sign and Peripheral rim sign in Multiple Sclerosis
☑️Dual rim sign in abscess
☑️Superficial siderosis
☑️Nigrosome 1 (Swallow tail) sign in Parkinson Disease
☑️Central vessel sign and Peripheral rim sign in Multiple Sclerosis
☑️Dual rim sign in abscess
☑️Superficial siderosis
8/ 𝗦𝗪𝗜 𝗶𝗻 𝗣𝗮𝗿𝗸𝗶𝗻𝘀𝗼𝗻 𝗱𝗶𝘀𝗲𝗮𝘀𝗲 (𝗣𝗗): High spatial resolution SWI images the nigrosome 1 (N1): the posterior substantia nigra which normally has high signal flanked by two linear hypointense regions: "swallow tail".
Neurodegeneration ➡️ loss of the bright spot
Neurodegeneration ➡️ loss of the bright spot

9/ Dementia with Lewy Bodies (DLB) and PD are on a spectrum since Lewy Body accumulation is seen in both and the distinction is made clinically. Loss of the N1 bright spot may differentiate DLB from Alzheimer Dementia (AD) and fronto-temporal lobar degeneration (FTLD):

10/ Multiple Sclerosis (MS) is a demyelinating disorder caused by perivenular inflammation. 𝗖𝗲𝗻𝘁𝗿𝗮𝗹 𝘃𝗲𝘀𝘀𝗲𝗹 𝘀𝗶𝗴𝗻 can be used to differentiate MS lesions (figure B) from vascular (or other) white matter lesions (figure A).

11/ Peripheral Rim Sign: A hypointense rim on SWI reflects iron deposition in macrophages in chronically active MS lesions. This has been linked to a worse clinical prognosis. The MS patient imaged below shows a T2 hyperintense lesion (A) demonstrating a peripheral rim sign (B).

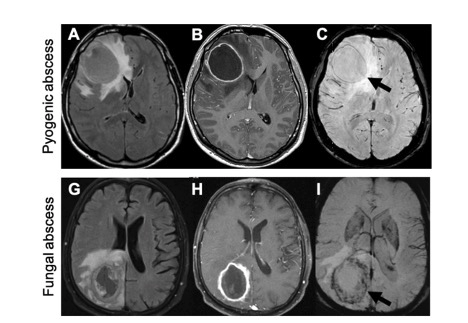
12/ Abscess: Dual rim sign, defined as a combination of hypointense and hyperintense rim, is a diagnostic sign in favor of pyogenic abscess (panel C) while fungal abscess classically shows peripheral hypointensity without dual rim (panel I).
13/ Superficial siderosis is linear signal loss following the pia from deposition of hemosiderin along the leptomeninges and can create a tram-track sign (below) when on both sides of a sulcus. It can be seen in trauma and cerebral amyloid angiopathy, amongst other etiologies.

14/ SUMMARY:
☝️SWI can distinguish microbleeds from microcalcs.
☝️Loss of the “Swallow Tail" suggests Parkinson disease or Dementia with Lewy Bodies
☝️Central vessel or Peripheral rim signs suggest MS rather than vascular lesion
☝️Dual rim suggests pyogenic > fungal abscess.
☝️SWI can distinguish microbleeds from microcalcs.
☝️Loss of the “Swallow Tail" suggests Parkinson disease or Dementia with Lewy Bodies
☝️Central vessel or Peripheral rim signs suggest MS rather than vascular lesion
☝️Dual rim suggests pyogenic > fungal abscess.
15/ Check out more detailed technical considerations and clinical applications of susceptibility weighted imaging with clinical neuro applications here:
pubs.rsna.org/doi/10.1148/ra…
@RSNA #RadinTraining @radiology_rsna
pubs.rsna.org/doi/10.1148/ra…
@RSNA #RadinTraining @radiology_rsna
• • •
Missing some Tweet in this thread? You can try to
force a refresh