1/ You've got feedback to give. But how to deliver it?
Hey #MedTwitter & #MedEd Friends!
We are the #MedEdTwagTeam, back again for another #TweetorialTuesday! 🙏 to all who follow, enjoy, and share!
Follow: @GStetsonMD, @JenniferSpicer4, & @MedEdTwagTeam to stay #UpToDate
Hey #MedTwitter & #MedEd Friends!
We are the #MedEdTwagTeam, back again for another #TweetorialTuesday! 🙏 to all who follow, enjoy, and share!
Follow: @GStetsonMD, @JenniferSpicer4, & @MedEdTwagTeam to stay #UpToDate

2/ We have reached Week 4 in our #Feedback threads.
Last week, @JenniferSpicer4 taught us all about the components of effective feedback, including setting, timing, specificity, frequency, and more.
This week we will talk about the two main methods of feedback “delivery.”
Last week, @JenniferSpicer4 taught us all about the components of effective feedback, including setting, timing, specificity, frequency, and more.
This week we will talk about the two main methods of feedback “delivery.”

3/ So the two main methods are a “download” and a “dialogue.” What do these terms mean?

4/ Last week, our friend @scotter joined the conversation and perfectly set us up to talk about the ”download.”
Much appreciated!!!
Much appreciated!!!

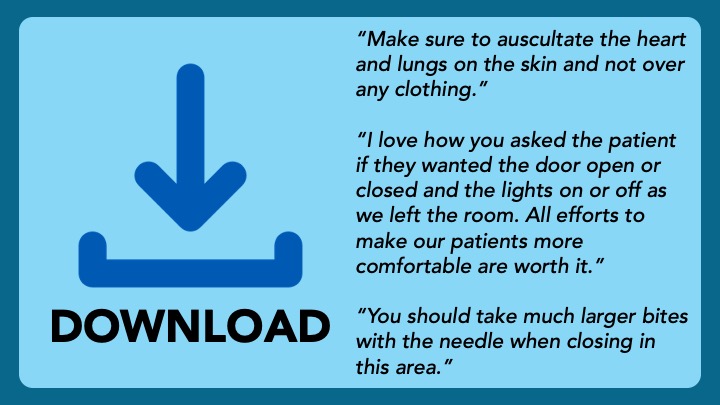
5/ When I say “download”, I mean a unidirectional information transfer from the teacher to the learner.
This is a great tool when the feedback is just one nugget, and the stakes are low. Examples:
This is a great tool when the feedback is just one nugget, and the stakes are low. Examples:
6/ However, the download works well only if implemented using the principles we have talked about over the last two weeks:
1⃣ Trust via a relationship.
2⃣ 4:1 Reinforcing:Modifying
3⃣ Setting, frequency, timing, etc.
See how we are scaffolding this material? #MedEdMagic
1⃣ Trust via a relationship.
2⃣ 4:1 Reinforcing:Modifying
3⃣ Setting, frequency, timing, etc.
See how we are scaffolding this material? #MedEdMagic
7/ Another #MedTwitter friend, @csdaisysmith, set us up perfectly to talk about the next tool, the “dialogue”. Thanks so much!!!

8/ A feedback “dialogue”, or conversation, should occur for anything complicated, or that might evoke an emotional response.
I employ “The ART of Feedback”, a skill learned from my mentor @calvinchou (of @UCSF, @SFVAMC & @ACHonline) who literally wrote the book(s) on #Feedback.
I employ “The ART of Feedback”, a skill learned from my mentor @calvinchou (of @UCSF, @SFVAMC & @ACHonline) who literally wrote the book(s) on #Feedback.
9/ Let’s break down “The ART of Feedback”, step-by-step.
Step 1⃣ – ASK the learner for their reflections. This can be on anything: a presentation, a patient encounter, a bed-side procedure, their ability to meet their learning goals, etc.
Step 1⃣ – ASK the learner for their reflections. This can be on anything: a presentation, a patient encounter, a bed-side procedure, their ability to meet their learning goals, etc.

10/ Step 2⃣ – REFLECT on what the learner said. Paraphrase their response to Step 1, and react to what they said, positive or negative.
▶️ If their reflection was generally positive, help them celebrate.
▶️ If their reflection was more critical, empathize.
▶️ If their reflection was generally positive, help them celebrate.
▶️ If their reflection was more critical, empathize.

11/ Step 3⃣ – TELL your learner your feedback, keeping in mind their personal interpretation.
▶️ If they were too hard on themselves, focus on the positives.
▶️ If they didn’t notice an opportunity to grow, make it clear using specific examples.
▶️ If they were too hard on themselves, focus on the positives.
▶️ If they didn’t notice an opportunity to grow, make it clear using specific examples.

12/ Step 4⃣ – Ask again! See how your feedback landed.
Do they agree? Any further thoughts? Do they disagree?
This might be the last step if you two are on the same page. If not, may need repeat steps 2 & 3.
Do they agree? Any further thoughts? Do they disagree?
This might be the last step if you two are on the same page. If not, may need repeat steps 2 & 3.
13/ The ART of Feedback may seem like a lot. But with practice, you and your learners can get fast.
I have gotten to the point where I can do this process in 2-3 minutes, allowing me to do it once/day/learner.
I have gotten to the point where I can do this process in 2-3 minutes, allowing me to do it once/day/learner.
14/ Thanks for joining us, friends. We are so glad you have been enjoying our threads. Please, leave any questions or thoughts in the comments.
Next week, I will be back to expand on today’s topic when we discuss #FormativeFeedback.
Have a great week!
Next week, I will be back to expand on today’s topic when we discuss #FormativeFeedback.
Have a great week!

• • •
Missing some Tweet in this thread? You can try to
force a refresh