
Excited to have @siddharth_dugar from @ClevelandClinic give the #MetroEUS Ultrasound Lecture today about Critical Care ECHO. #POCUS #FOAMed #FOAMus #EchoFirst @MetroHealth_EM @metrohealthCLE @RJonesSonoEM @mtabbut @SLWerner_EM @DianeGramer 

Goal and benefit of POCUS is to rapidly narrow the differential diagnosis through asking and answering defined clinical questions.

POCUS will narrow the differential more rapidly

Also remember to look at your structure through multiple planes. One view is no view.

Ultrasound Protocol for shock

Start looking for an effusion. Differentiate pericardial vs pleural effusion. Key: look for the descending thoracic aorta in the PSLA view. Fluid above = pericardial (blue), fluid up to and below = pleural (green)


Grading a pericardial effusion. Measure the size of the effusion in diastole.

Does the patient have tamponade? Look at the IVC. If small, then likely no tamponade. If enlarged, need to look for other factors.

Other factors to assess for tamponade are RA systolic collapse, RV diastolic collapse.


RA/RV collapse to assess for tamponade is limited in patients with advanced pulmonary hypertension due to high RA/RV pressures. Teaching Pearl: look at the LA free wall as this is the lowest pressure chamber. #MicDrop @siddharth_dugar #FOAMus

Next on the protocol. Look at the RV. Is it normal size? Is it dilated relative to LV.

Look for other signs of RV strain: Plethoric IVC, Flattened septum (D sign). If you find DVT or see McConnell's sign (remember patient in shock), then PE is your major concern.


Next move to the LV. Start with looking at global LV function: Hyperdynamic, normal hypokinetic.

As a general rule of thumb for patients in shock - though there are certainly exceptions.
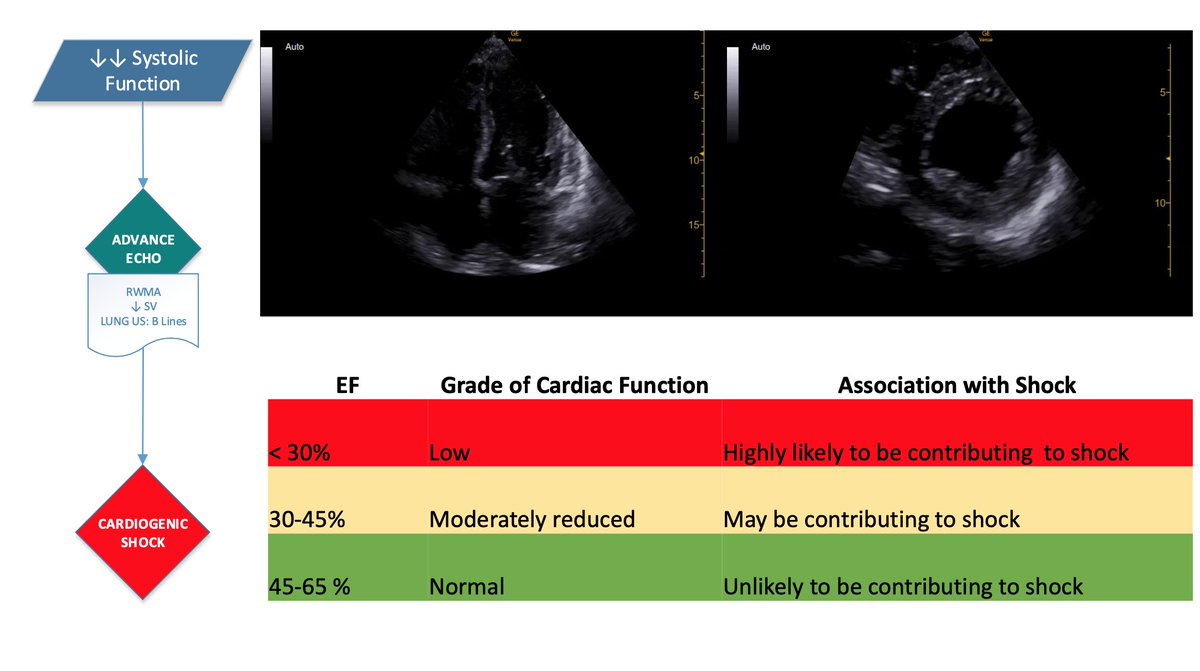
When assessing cardiogenic shock, look next at the lungs for B lines.

What about patients who are normal dynamic or hyperdynamic?

Still can't find the cause of shock? Look for severe valvular regurgitation, LVOT obstruction, aortic dissections.

And don't forget about tension pneumothorax.

• • •
Missing some Tweet in this thread? You can try to
force a refresh


