
People often make the claim that, during the COVID-19 pandemic, we have "failed to protect the elderly"
While initially this was definitely true (April/March 2020), I'm not sure the claim is accurate past that 1/n
While initially this was definitely true (April/March 2020), I'm not sure the claim is accurate past that 1/n

2/n I'm basing my opinion here on seroprevalence data. This is basically data looking at who has antibodies to COVID-19, and therefore who was previously infected
We reviewed 100s of studies for our IFR paper. What did they show? link.springer.com/article/10.100…
We reviewed 100s of studies for our IFR paper. What did they show? link.springer.com/article/10.100…
3/n Well, not all of them looked at the age-stratified rates of infection
But of those that DID, an interesting pattern emerges
But of those that DID, an interesting pattern emerges
3.5/n (Note: this is excluding low-quality seroprevalence estimates with selection bias issues. These cannot be trusted to give us an accurate estimation of infection rates by age)
4/n For example, take REACT-2, a massive antibody prevalence study from the UK
They found substantially FEWER people had been infected in older age groups than younger ones
They found substantially FEWER people had been infected in older age groups than younger ones

5/n If you look at our supplementary appendix, where we give age-stratified prevalence figures for every study, you see a similar pattern in many places...



6/n ...with some VERY notable exceptions!
But remember, these are seroprevalence estimates taken in Italy and Spain in April 2020
But remember, these are seroprevalence estimates taken in Italy and Spain in April 2020


7/n Indeed, places that were hit really early on seem to show the opposite pattern
Here are the results for the small Italian town Castiglione D'Adda. Older people were MORE likely to be infected
Here are the results for the small Italian town Castiglione D'Adda. Older people were MORE likely to be infected

8/n But that's the thing - in the very early epidemic, people did not protect the elderly
However, what the evidence appears to show is that this was a relatively short-lived phenomenon
However, what the evidence appears to show is that this was a relatively short-lived phenomenon
9/n While this is somewhat speculative (mostly my opinion) I think it's fair to say that after the tragedy of the early first wave, most places implemented policies that substantially reduced the number of COVID-19 infections of elderly people
10/n All over the world, people took more care with their grandparents, aged care centres curtailed visitation, and generally we were all more aware of the danger to the elderly
11/n This is seen in the numbers - many places that were hit even a few weeks later than Italy/Spain had lower infection rates in older people than younger
12/n Even within countries, I suspect there may have been an impact
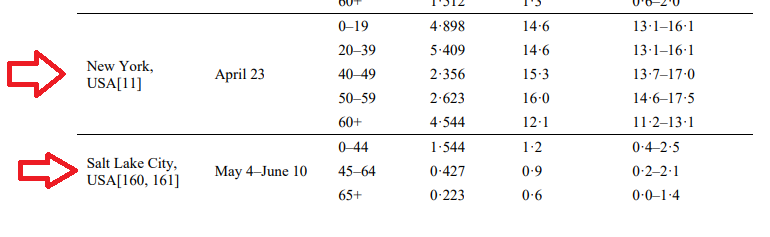
For example, New York had ~some~ reduction in infection in older people, but Utah had a big reduction
For example, New York had ~some~ reduction in infection in older people, but Utah had a big reduction
13/n Like I said, all of this is pretty speculative. It's hard to say how much we managed to protect older people because often the seroprevalence data is not very good
14/n That being said, when we look at good quality seroprevalence estimates, in almost all cases after the initial surge it looks like we did in fact protect elderly people (at least to some extent)
15/n Yes, elderly people have died more from COVID-19, but that's an obvious consequence of the age-stratified IFR. If lots of people get infected, lots of old people will be infected by default
16/n I think it is reasonable to say that in most places we HAVE protected the elderly to a great degree, and we have still suffered the consequences when the pandemic got out of control
• • •
Missing some Tweet in this thread? You can try to
force a refresh




