1/
Attending: “But never anticoagulation for an intracranial dissection!”
Me as a resident: “Of course. Totally!”
Also me ⬇️: [googling “where do the internal carotid arteries and vertebral arteries become intracranial?”]
Feel familiar? A #tweetorial @MedTweetorials
Attending: “But never anticoagulation for an intracranial dissection!”
Me as a resident: “Of course. Totally!”
Also me ⬇️: [googling “where do the internal carotid arteries and vertebral arteries become intracranial?”]
Feel familiar? A #tweetorial @MedTweetorials
2/
With the TREAT-CAD trial, lots of talk about dissection treatment. Whether your team anti-platelets or team anticoagulation (🙋🏻 Must. Give. Heparin (@MGHNeurology) 4 ever. I know you feel this, @namorris!) consideration about the location of dissection is possibly important.
With the TREAT-CAD trial, lots of talk about dissection treatment. Whether your team anti-platelets or team anticoagulation (🙋🏻 Must. Give. Heparin (@MGHNeurology) 4 ever. I know you feel this, @namorris!) consideration about the location of dissection is possibly important.
3/
Also, regardless of your team… TREAT-CAD was not able to demonstrate non-inferiority of ASA, just saying.
Aspirin versus anticoagulation in cervical artery dissection (TREAT-CAD): an open-label, randomised, non-inferiorit… pubmed.ncbi.nlm.nih.gov/33765420/
Also, regardless of your team… TREAT-CAD was not able to demonstrate non-inferiority of ASA, just saying.
Aspirin versus anticoagulation in cervical artery dissection (TREAT-CAD): an open-label, randomised, non-inferiorit… pubmed.ncbi.nlm.nih.gov/33765420/
4/
K, back to the question.
So, when do the verts become intracranial? This is fairly straight forward -- as it passes through the transverse foramen of C1 marking the transition between V3 and V4 segments.
K, back to the question.
So, when do the verts become intracranial? This is fairly straight forward -- as it passes through the transverse foramen of C1 marking the transition between V3 and V4 segments.
5/
The carotids are more complicated. The most commonly used naming system was described by Alain Bouthillier in 1996.
Segments of the Internal Carotid Artery: A New Classification …demic-oup-com.proxy.library.emory.edu/neurosurgery/a…
The carotids are more complicated. The most commonly used naming system was described by Alain Bouthillier in 1996.
Segments of the Internal Carotid Artery: A New Classification …demic-oup-com.proxy.library.emory.edu/neurosurgery/a…
6/
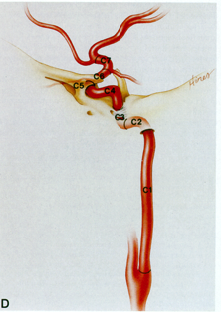
In reading this I developed an appreciation for the incredible anatomical effort that went into describing these segments. The illustrations in this manuscript are INCREDIBLE
C1-cervical, C2-Petrous, C3- Lacerum, C4-Cavernous, C5-Clinoid, C6-Ophthalmic, C7-Communicating
In reading this I developed an appreciation for the incredible anatomical effort that went into describing these segments. The illustrations in this manuscript are INCREDIBLE
C1-cervical, C2-Petrous, C3- Lacerum, C4-Cavernous, C5-Clinoid, C6-Ophthalmic, C7-Communicating
7/
Most authors consider the carotid intracranial as it transitions from the cervical segment into the carotid canal in the C2-petrous segment. HOWEVER, the carotid is not *intradural* until it traverses the distal dural ring at the end of the clinoid segment:
Most authors consider the carotid intracranial as it transitions from the cervical segment into the carotid canal in the C2-petrous segment. HOWEVER, the carotid is not *intradural* until it traverses the distal dural ring at the end of the clinoid segment:

8/
After passing the distal dural ring, extension of dissection could result in subarachnoid hemorrhage.
Note: While SAH may not be a complication of more proximal dissection, a carotid-cavernous fistula could result from a subadventitial dissection in the C4-Cavernous seg.😱
After passing the distal dural ring, extension of dissection could result in subarachnoid hemorrhage.
Note: While SAH may not be a complication of more proximal dissection, a carotid-cavernous fistula could result from a subadventitial dissection in the C4-Cavernous seg.😱
9/
Does SAH develop after the initial injury though and is it really not safe to anticoagulation a patient with an intracranial dissection?
The answer is it probably doesn’t happen often, and it’s probably safe.
Does SAH develop after the initial injury though and is it really not safe to anticoagulation a patient with an intracranial dissection?
The answer is it probably doesn’t happen often, and it’s probably safe.
10/
In one large case series of 80 patients with intracranial dissection, with no radiographic or clinical concern for presenting SAH, no cases of SAH were observed despite treatment with anticoagulation.
ahajournals.org/doi/10.1161/st…
In one large case series of 80 patients with intracranial dissection, with no radiographic or clinical concern for presenting SAH, no cases of SAH were observed despite treatment with anticoagulation.
ahajournals.org/doi/10.1161/st…
11/
However, I still often want to know.
Many images exist that demonstrate the segments of the carotid/verts. But, none that I found had them in as reformatted CTA MIPS next to the bony segments, which is what I wanted.
So, I made some for the #acuteneurologysurvivalguide!
However, I still often want to know.
Many images exist that demonstrate the segments of the carotid/verts. But, none that I found had them in as reformatted CTA MIPS next to the bony segments, which is what I wanted.
So, I made some for the #acuteneurologysurvivalguide!

12/
If you want to do more reading, both radiopaedia.org and Neuroangio.org have excellent articles. Highly recommend!
#neurotwitter #acuteneurologysurvivalguide #endneurophobia #MedEd
Thoughts? @namorrismd @AaronLBerkowitz @Capt_Ammonia @sauravmed @rwregen
If you want to do more reading, both radiopaedia.org and Neuroangio.org have excellent articles. Highly recommend!
#neurotwitter #acuteneurologysurvivalguide #endneurophobia #MedEd
Thoughts? @namorrismd @AaronLBerkowitz @Capt_Ammonia @sauravmed @rwregen
• • •
Missing some Tweet in this thread? You can try to
force a refresh