ANYBODY in Ontario who lives in a high burden neighbourhood who is 18 years and older will be eligible for #COVID19 vaccination.
This will help essential workers, families, communities, etc.
A very smart move.
This will help essential workers, families, communities, etc.
A very smart move.
Mobile teams to help bring the vaccine to the people. This will happen in workplaces, congregate settings, dense urban areas, etc.
1. More access to vaccine.
2. Lower barriers to vaccination.
1. More access to vaccine.
2. Lower barriers to vaccination.
This is the part of the Phase 2 Vaccine roll out that prioritizes communities at greater risk.
Link: bit.ly/2R5Ffaj
Link: bit.ly/2R5Ffaj

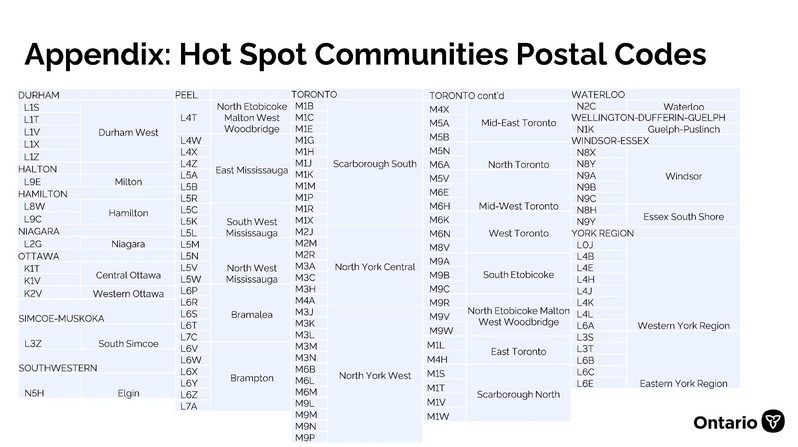
These are the actual postal codes that will have priority vaccination.
IMPLEMENTATION is key though.
Because there is still a shortage of vaccines, this will be implemented through mobile vaccine teams and pop-up clinics focused in "high-risk congregate settings, residential buildings, faith-based locations, & locations occupied by large employers"
Because there is still a shortage of vaccines, this will be implemented through mobile vaccine teams and pop-up clinics focused in "high-risk congregate settings, residential buildings, faith-based locations, & locations occupied by large employers"
"Vaccinations will commence during the April break starting with priority neighborhoods in Toronto and Peel, then rolling out to priority neighborhoods in other hot spot regions, including York, Ottawa, Hamilton, Halton & Durham."
• • •
Missing some Tweet in this thread? You can try to
force a refresh