On today's episode of “PUTTING YOUR IGNORANCE ON DISPLAY!” What does a partial- and full-thickness tear look like? Today, I had a sudden understanding/facepalming moment...
@Retlouping @ShoulderGeek1 @DrJN_SportsMed @JeremyLewisPT
@Retlouping @ShoulderGeek1 @DrJN_SportsMed @JeremyLewisPT
Here was my thought, how can a full-thickness tear be small-medium-large when its FULL thickness? Full is full, how can it be small? This might be obvious to u...
Here was my internal image of what a partial and full-thickness tear looked like.
Here was my internal image of what a partial and full-thickness tear looked like.

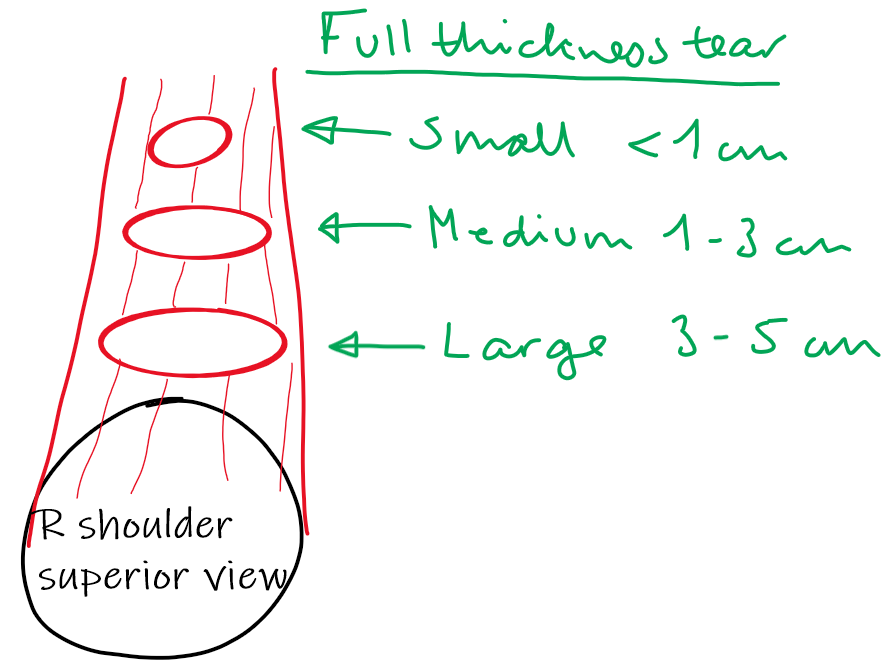
Of course, a full-thickness tear can look like the picture above, but here is an image of the “correct” way to look at it. The first picture is a superior view of the right shoulder with the supraspinatus. The second is an anterior view. The two images are of the same two tears.

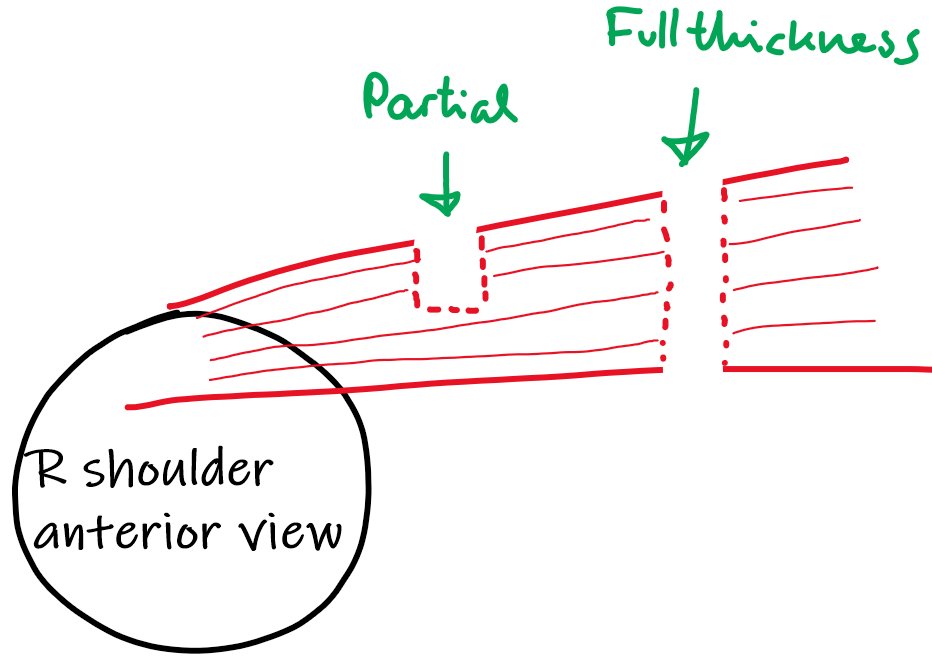
Full-thickness describes a HOLE through the FULL THICKNESS of the muscle belly. It describes a superior-to-inferior tear pattern, NOT an anterior-to-posterior tear pattern (like picture 1)
Now it becomes obvious how a full-thickness tear can be different sizes. It's just the diameter of the hole.
I would be very interested to hear if anyone had/have the same misunderstanding.
Also, praise for my painting skills would not go amiss 😁
Also, praise for my painting skills would not go amiss 😁
@threadreaderapp unroll
• • •
Missing some Tweet in this thread? You can try to
force a refresh