Sideroblastic anemias!
[Tweetorial]
Pathological iron deposition in mitochondria of erythroid precursors
Pathologic finding
🚫a specific diagnosis!
Broad classification of sideroblastic anemias.
1. Congenital
-Syndromic
-Non-syndromic
2. Acquired
-Clonal
-Metabolic
-Drugs
[Tweetorial]
Pathological iron deposition in mitochondria of erythroid precursors
Pathologic finding
🚫a specific diagnosis!
Broad classification of sideroblastic anemias.
1. Congenital
-Syndromic
-Non-syndromic
2. Acquired
-Clonal
-Metabolic
-Drugs

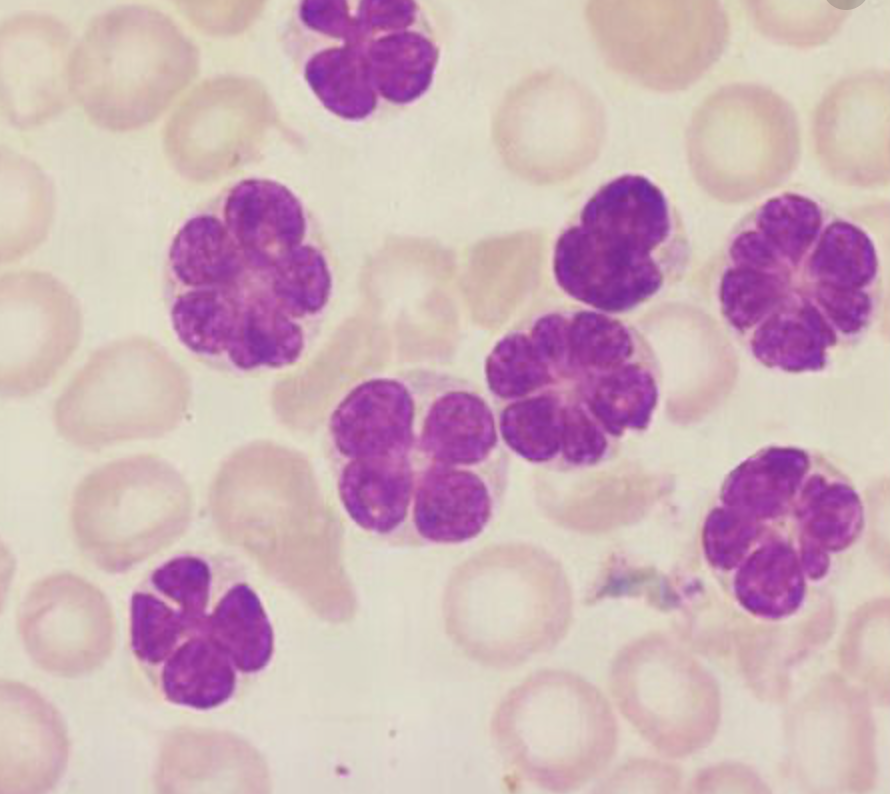
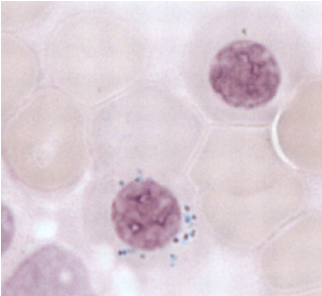
WHO defined types of sideroblasts
Type 1: <5 siderotic granules in cytoplasm.
Type 2: ≥5 granules but no perinuclear distribution.
Type 3 = ringed sideroblast: ≥ 5 granules in a perinuclear position, surrounding nucleus or encompassing one third of nuclear circumference.
Type 1: <5 siderotic granules in cytoplasm.
Type 2: ≥5 granules but no perinuclear distribution.
Type 3 = ringed sideroblast: ≥ 5 granules in a perinuclear position, surrounding nucleus or encompassing one third of nuclear circumference.


Mitochondria Anatomy
Sideroblasts = Mitochondria problems
Outer membrane
-Porins for proteins
Intermembrane space
Inner membrane
-Oxidative phosphorylation
-ATP synthase
Cristae
-Expand membrane space
Matrix
-Mitochondrial DNA
-TCA cycle
-Heme synthesis
-Oxidaiton of lipids
Sideroblasts = Mitochondria problems
Outer membrane
-Porins for proteins
Intermembrane space
Inner membrane
-Oxidative phosphorylation
-ATP synthase
Cristae
-Expand membrane space
Matrix
-Mitochondrial DNA
-TCA cycle
-Heme synthesis
-Oxidaiton of lipids

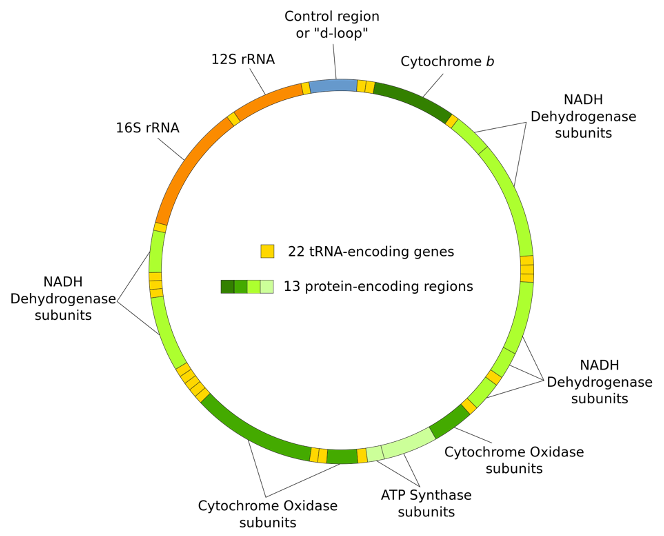
Mitochondrial Genetics
Maternally inherited
5-10 copies of 16569 BP circular DNA per mitochondria
13 mRNAs (respiratory complexes)
22 mt-tRNAs
2 mt-rRNAs
Maternally inherited
5-10 copies of 16569 BP circular DNA per mitochondria
13 mRNAs (respiratory complexes)
22 mt-tRNAs
2 mt-rRNAs
Mitochondria Trafficking
Lots of proteins used in mito not coded by mito DNA
(> 1000 proteins) trafficked:
Through outer membrane (TOMs)
Through intermembrane space (TIMs)
Proteins trafficked through:
All of Krebs cycle
4 heme synthesis enzymes
All mitochondrial transporters
Lots of proteins used in mito not coded by mito DNA
(> 1000 proteins) trafficked:
Through outer membrane (TOMs)
Through intermembrane space (TIMs)
Proteins trafficked through:
All of Krebs cycle
4 heme synthesis enzymes
All mitochondrial transporters

Congenital Sideroblastic Anemias
Heme synthesis defects
-XLSA
Mitochondrial transporter defects
-SLC25A38
-Thiamine responsive megaloblastic anemia
Fe-S biogenesis defects
-X-linked sideroblastic anemia with ataxia
Mitochondrial protein synthesis defects
-Pearson’s syndrome
Heme synthesis defects
-XLSA
Mitochondrial transporter defects
-SLC25A38
-Thiamine responsive megaloblastic anemia
Fe-S biogenesis defects
-X-linked sideroblastic anemia with ataxia
Mitochondrial protein synthesis defects
-Pearson’s syndrome
X-linked Sideroblastic Anemia (XLSA)
Mutations in ALAS2
-First step in heme synthesis!
-Occurs in mitochondria
-Over 80 mutations
-Catalytic domain
-Reduced enzymatic activity
Mutations in ALAS2
-First step in heme synthesis!
-Occurs in mitochondria
-Over 80 mutations
-Catalytic domain
-Reduced enzymatic activity

X-linked Sideroblastic Anemia (XLSA)
Males (age 40)
Rare female 2/2 skewed X inactivation
Transfusion dependence rare
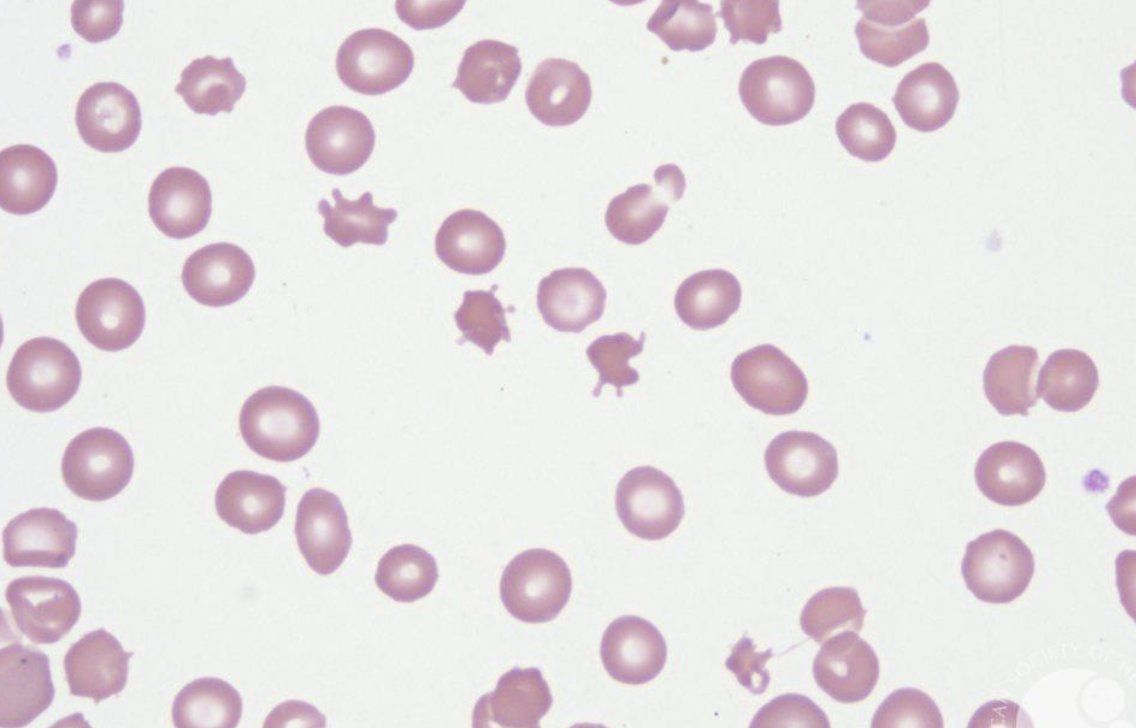
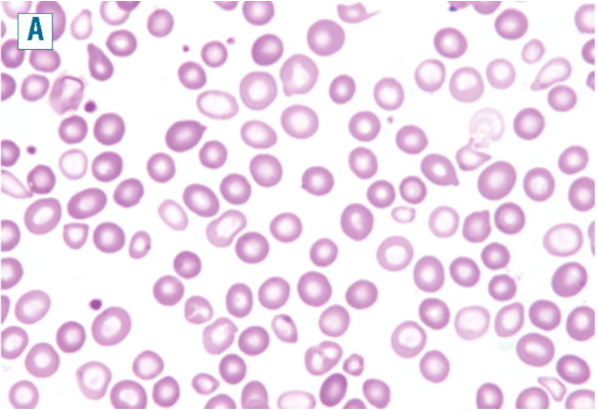
Smear:
Microcytic
Hypochromic
Dimorphic (⬆️RDW)
Pappenheimer bodies
Treatment:
Pyridoxine(B6) > 50 mg day
Mutations altering pyridoxine binding are responsive
Males (age 40)
Rare female 2/2 skewed X inactivation
Transfusion dependence rare
Smear:
Microcytic
Hypochromic
Dimorphic (⬆️RDW)
Pappenheimer bodies
Treatment:
Pyridoxine(B6) > 50 mg day
Mutations altering pyridoxine binding are responsive

Sideroblastic anemia 2/2 mutations in SLC25A38
Severe hypochromic anemia resembles XLSA but lacked ALAS2 mutation.
Anemia first weeks of life
Unresponsive to B6
Chronic transfusion support
SLC25A38 mutations
Inner mito membrane
Transports ALA out of mito
Glycine import to mito
Severe hypochromic anemia resembles XLSA but lacked ALAS2 mutation.
Anemia first weeks of life
Unresponsive to B6
Chronic transfusion support
SLC25A38 mutations
Inner mito membrane
Transports ALA out of mito
Glycine import to mito

Thiamine (B1) Responsive Megaloblastic Anemia
Sideroblastic+Megaloblastic!
Mutation mitochondria B1 transp SLC19A2
B1 cofactor mitochondria enzymes:
Transketolase = ribose for nucleotide
PDH = SucCoA for heme synthesis
⬇️B1->
⬇️Nucleotide = megaloblastic
⬇️Heme = sideroblastic
Sideroblastic+Megaloblastic!
Mutation mitochondria B1 transp SLC19A2
B1 cofactor mitochondria enzymes:
Transketolase = ribose for nucleotide
PDH = SucCoA for heme synthesis
⬇️B1->
⬇️Nucleotide = megaloblastic
⬇️Heme = sideroblastic

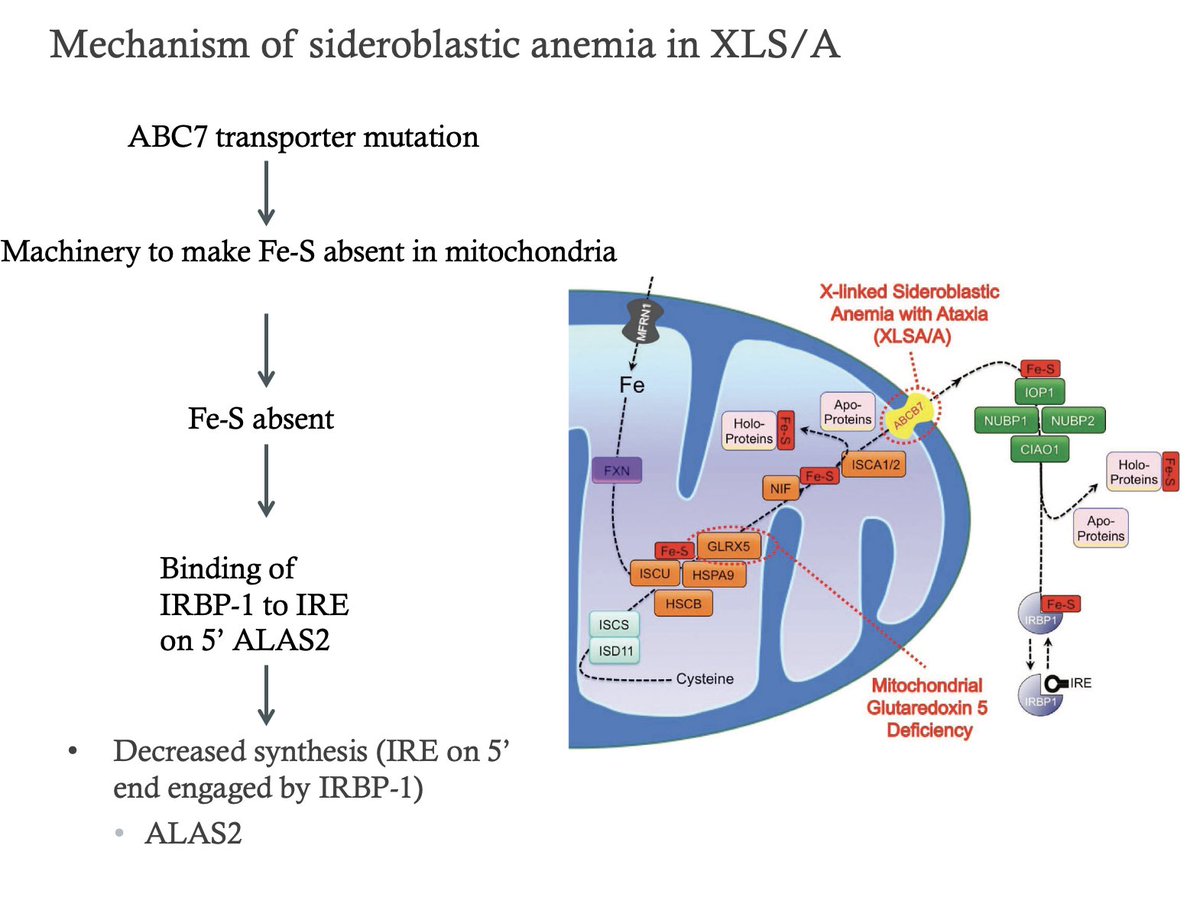
X-linked sideroblastic anemia with ataxia (XLSA/A)
Early onset motor delay, spinocerebellar hypoplasia
Ataxia with severe cerebellar hypoplasia
Mild sideroblastic anemia
Mutation ABC7 transporters:
Transports components involved in construction of Fe-S clusters.
Early onset motor delay, spinocerebellar hypoplasia
Ataxia with severe cerebellar hypoplasia
Mild sideroblastic anemia
Mutation ABC7 transporters:
Transports components involved in construction of Fe-S clusters.
Board Review Question!
What is your differential for an infant with anemia and pancreatic insufficiency?
1. Shwachman-Diamond syndrome
2. Pearson’s syndrome
Pearl: Pearson’s syndrome has ringed sideroblasts while Shwachman-Diamond syndrome does not.
What is your differential for an infant with anemia and pancreatic insufficiency?
1. Shwachman-Diamond syndrome
2. Pearson’s syndrome
Pearl: Pearson’s syndrome has ringed sideroblasts while Shwachman-Diamond syndrome does not.
Pearson's syndrome = Mitochondrial DNA
Presents in infants
-Lactic acidosis
-Pancreatic insufficiency
-Myopathy
Spectrum of Kearns-Sayre syndrome
Pancytopenia, ringed sideroblasts
Vacuolization hematopoietic precursors
Maternally inherited
4977 bp deletion mitochondrial genome
Presents in infants
-Lactic acidosis
-Pancreatic insufficiency
-Myopathy
Spectrum of Kearns-Sayre syndrome
Pancytopenia, ringed sideroblasts
Vacuolization hematopoietic precursors
Maternally inherited
4977 bp deletion mitochondrial genome

Acquired Sideroblastic Anemia
Clonal
-RARS
-RARS-T
-RCMD-RS
Metabolic
-Copper deficiency
-Zinc toxicity
Drugs
-Chloramphenicol
-INH
-Linezolid
Alcoholism
Hypothermia
Clonal
-RARS
-RARS-T
-RCMD-RS
Metabolic
-Copper deficiency
-Zinc toxicity
Drugs
-Chloramphenicol
-INH
-Linezolid
Alcoholism
Hypothermia
Clonal
RARS: dysplasia confined to the erythroid cell lineage.
-All have SF3B1 mutation
RARS-T: Anemia+thrombocytosis
-SF3B1+JAK2 V617F which frequently has the
RCMD-RS: MDS with additional dysplastic features involving granulopoiesis and/or megakaryopoiesis.
-SF3B1
RARS: dysplasia confined to the erythroid cell lineage.
-All have SF3B1 mutation
RARS-T: Anemia+thrombocytosis
-SF3B1+JAK2 V617F which frequently has the
RCMD-RS: MDS with additional dysplastic features involving granulopoiesis and/or megakaryopoiesis.
-SF3B1


Copper deficiency
⬇️Cu disrupts iron metabolism
⬇️Intestinal Fe absorption 2/2 lack of ceruloplasmin and ferroxidase function in haphaestin
⬇️ferrous iron in mitochondria 2/2 ⬇️cytochrome c oxidase (necessary for heme synthesis)
⬆️Zinc excess causes ⬇️copper
-⬇️ Cu absorption
⬇️Cu disrupts iron metabolism
⬇️Intestinal Fe absorption 2/2 lack of ceruloplasmin and ferroxidase function in haphaestin
⬇️ferrous iron in mitochondria 2/2 ⬇️cytochrome c oxidase (necessary for heme synthesis)
⬆️Zinc excess causes ⬇️copper
-⬇️ Cu absorption

Drugs
INH: Interferes with B6 metabolism
Depletes ALAS2 of pyridoxal phosphate
Chloramphenicol/Linezolid: Inhibits bacterial ribosomes:
⬇️Mitochondrial rRNA
INH: Interferes with B6 metabolism
Depletes ALAS2 of pyridoxal phosphate
Chloramphenicol/Linezolid: Inhibits bacterial ribosomes:
⬇️Mitochondrial rRNA

My clinical approach to sideroblastic anemias

Pearls
Anemia usually mild 9-12 for all except:
SLC25A38 (severe and young age)
WBC and plt count usually normal except:
Pearson’s syndrome (pancytopenia)
Copper deficiency (neutropenia)
RARS-T (thrombocytosis)
XLSA in female mimics RARS!
High MCV
Dimorphic RBCs
Anemia usually mild 9-12 for all except:
SLC25A38 (severe and young age)
WBC and plt count usually normal except:
Pearson’s syndrome (pancytopenia)
Copper deficiency (neutropenia)
RARS-T (thrombocytosis)
XLSA in female mimics RARS!
High MCV
Dimorphic RBCs

Treatment
General principles
Avoid unnecessary transfusion
Iron overload
Iron chelation therapy
Phlebotomy
XLSA = high dose B6
EtoH = Stop the booze
Copper deficiency = Parental or high dose PO copper
RARS = EPO, luspatercept
INH = Supplement with B6
General principles
Avoid unnecessary transfusion
Iron overload
Iron chelation therapy
Phlebotomy
XLSA = high dose B6
EtoH = Stop the booze
Copper deficiency = Parental or high dose PO copper
RARS = EPO, luspatercept
INH = Supplement with B6
• • •
Missing some Tweet in this thread? You can try to
force a refresh