
💥Endocrine adverse effects of Immune Checkpoint Inhibitors - a brief Tweetorial for Nephrologists
A thread based on an article published in @NatureRevEndo
👉🏽 nature.com/articles/s4157…
#Onconephrology
1/
A thread based on an article published in @NatureRevEndo
👉🏽 nature.com/articles/s4157…
#Onconephrology
1/
⚡️It important for Nephrologists to be familiar with immune checkpoint inhibitor induced endocrinopathies as thyroid, pituitary & adrenal disorders can present with👇🏽
-Hyponatremia
-Hyperkalemia
-Metabolic acidosis
-Hypotension
2/
-Hyponatremia
-Hyperkalemia
-Metabolic acidosis
-Hypotension
2/
⚡️Immune checkpoint inhibitors (ICIs) are monoclonal antibodies that target immune checkpoint proteins:
-Cytotoxic T lymphocyte antigen 4 (CTLA4)
-Programmed cell death 1 (PD1)
-Programmed cell death ligand 1 (PDL1)
3/
-Cytotoxic T lymphocyte antigen 4 (CTLA4)
-Programmed cell death 1 (PD1)
-Programmed cell death ligand 1 (PDL1)
3/
⚡️Immune checkpoint proteins (CTLA4, PD1, PDL1) are regulators of immune tolerance & prevent autoimmune responses in normal state
But cell surface expression of checkpoint proteins is ⬆️ in cancer cells & that is how cancer cells evade the immune system
4/
But cell surface expression of checkpoint proteins is ⬆️ in cancer cells & that is how cancer cells evade the immune system
4/
⚡️Hence ICIs are used for cancer Rx as they bind to & inhibit immune checkpoint proteins (CTLA4, PD1, PDL1) & target the signaling pathways related to
T-cell activation & exhaustion👇🏽
Currently ICIs are approved for use in 17 different types of cancer
5/
T-cell activation & exhaustion👇🏽
Currently ICIs are approved for use in 17 different types of cancer
5/

⚡️On one hand ICIs target cancer cells by targeting immune check point proteins
But recall that checkpoint proteins prevent autoimmunity therefore use of ICIs leads to removal of self-tolerance & auto-inflammation = immune related adverse events (irAEs)
6/
But recall that checkpoint proteins prevent autoimmunity therefore use of ICIs leads to removal of self-tolerance & auto-inflammation = immune related adverse events (irAEs)
6/
⚡️irAEs can affect any organ system with inflammatory manifestations
Most commonly affected organs are skin, colon, lungs, liver & thyroid
Some form of irAEs occur in up to 80-90% patients on ICIs
7/
Most commonly affected organs are skin, colon, lungs, liver & thyroid
Some form of irAEs occur in up to 80-90% patients on ICIs
7/
⚡️Endocrine adverse events can occur in up to 40% of patients treated with ICIs & can affect:
-Thyroid (most common): hypo- or hyperthyroidism
-Pituitary: hypophysitis
-Adrenal: adrenal insufficiency
-Pancreas: diabetes mellitus
👇🏽
8/
-Thyroid (most common): hypo- or hyperthyroidism
-Pituitary: hypophysitis
-Adrenal: adrenal insufficiency
-Pancreas: diabetes mellitus
👇🏽
8/

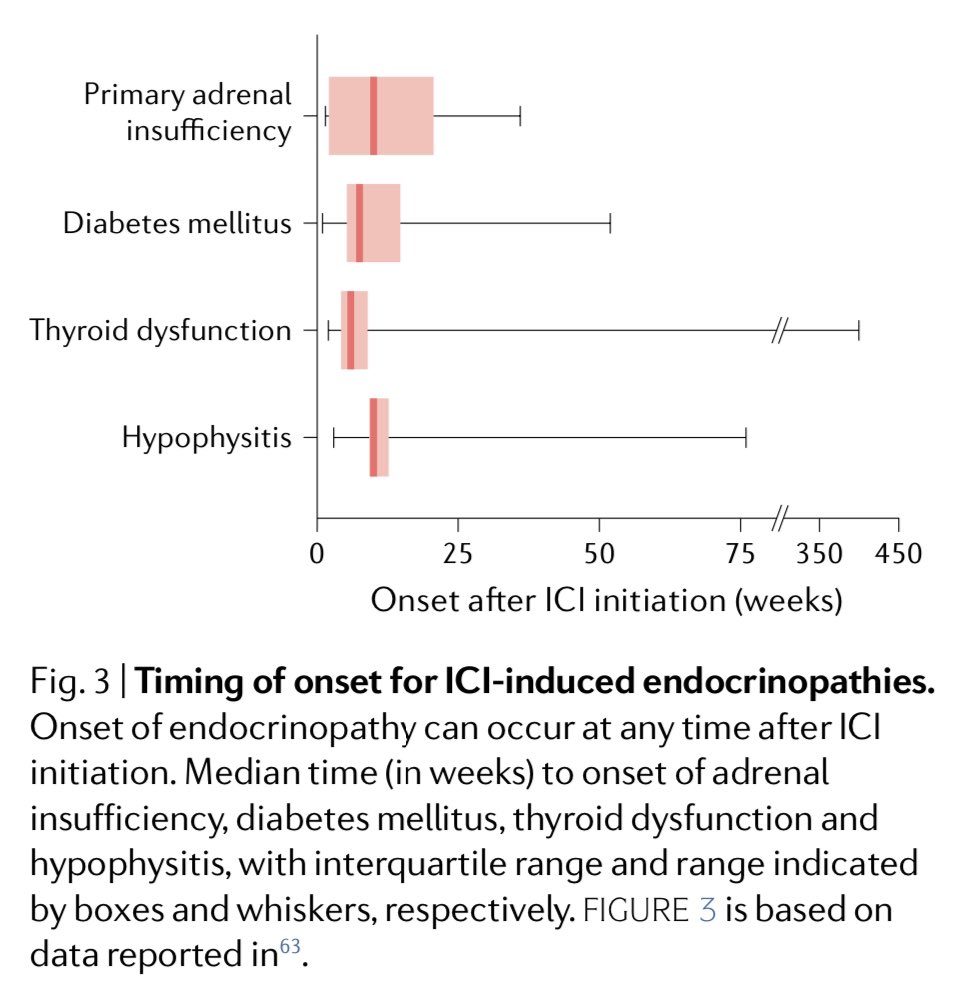
⚡️Endocrine adverse events due to ICIs typically present within 6-months of ICI initiation BUT they can be quite variable (even several months after cessation of ICIs)👇🏽
Key point is that ICI induced endocrinopathies are usually irreversible
9/
Key point is that ICI induced endocrinopathies are usually irreversible
9/
⚡️Why are ICI-induced endocrinopathies irreversible whereas inflammation in other organs due to ICIs is usually transient?
-One explanation is that immune activation by ICIs destroy most or all of the ‘small’ number of hormone producing cells
10/
-One explanation is that immune activation by ICIs destroy most or all of the ‘small’ number of hormone producing cells
10/
⚡️Hence ICI-induced endocrinopathies are permanent & are typically NOT treated with ICI discontinuation or with steroids
👆🏽This is different from how we Rx ICI-induced nephritis
ICI-induced endocrinopathies are treated with hormone replacement
11/
👆🏽This is different from how we Rx ICI-induced nephritis
ICI-induced endocrinopathies are treated with hormone replacement
11/
⚡️Most common ICI-induced endocrinopathy is thyroid toxicity
-Hypothyroidism is more common than hyperthyroidism
-Median time to onset is 6-weeks after ICI initiation but can occur at anytime
-More common with anti-PD1 or PDL1 than with anti-CTLA4
12/
-Hypothyroidism is more common than hyperthyroidism
-Median time to onset is 6-weeks after ICI initiation but can occur at anytime
-More common with anti-PD1 or PDL1 than with anti-CTLA4
12/
⬆️ TSH + ⬇️ FT4 = Primary hypothyroidism
⬇️ TSH + ⬇️ FT4 = Secondary hypothyroidism (assess for ICI-induced pituitary dysfunction: hyophysitis)
⬇️ TSH + ⬆️ FT4 = Primary hyperthyroidism (can occur due to ICI-induced thyroiditis)
13/
⬇️ TSH + ⬇️ FT4 = Secondary hypothyroidism (assess for ICI-induced pituitary dysfunction: hyophysitis)
⬇️ TSH + ⬆️ FT4 = Primary hyperthyroidism (can occur due to ICI-induced thyroiditis)
13/
⚡️Patients on ICIs should have thyroid function checked at least q8 wks
Thyroid hormone is used to Rx hypothyroidism
Thyroiditis associated thyrotoxicosis is Rx with supportive therapy
Graves dz Rx: anti-thyroid Rx, radioactive iodine or surgery
14/
Thyroid hormone is used to Rx hypothyroidism
Thyroiditis associated thyrotoxicosis is Rx with supportive therapy
Graves dz Rx: anti-thyroid Rx, radioactive iodine or surgery
14/
⚡️Note above that steroids are NOT used to treat ICI-induced thyroid diseases
-Another ICI-induced endocrinopathy is pituitary toxicity
Inflammation of the pituitary gland (hypophysitis) is very rare but it can occur in up to 10% of patients on ICIs
15/
-Another ICI-induced endocrinopathy is pituitary toxicity
Inflammation of the pituitary gland (hypophysitis) is very rare but it can occur in up to 10% of patients on ICIs
15/
⚡️Hyophysitis is more common with anti-CTLA4 than with anti-PD1 or anti-PDL1
Median time to presentation is 9-12 weeks after anti-CTL4 initiation & 26-weeks after anti-PD 1, anti-PDL1 initiation
Symptoms: headache, N/V, visual effects, fatigue, low BP
16/
Median time to presentation is 9-12 weeks after anti-CTL4 initiation & 26-weeks after anti-PD 1, anti-PDL1 initiation
Symptoms: headache, N/V, visual effects, fatigue, low BP
16/
⚡️ICI-induced hypophysitis can affect one or multiple hormonal axes
⬇️ACTH + ⬇️ cortisol
⬇️ TSH + ⬇️ FT4
⬇️ LH + ⬇️ FH + ⬇️sex hormones
Rx is hormone replacement
-Glucocorticoids or Thyroid or estrogen / testosterone based on underlying deficiency👇🏽
17/
⬇️ACTH + ⬇️ cortisol
⬇️ TSH + ⬇️ FT4
⬇️ LH + ⬇️ FH + ⬇️sex hormones
Rx is hormone replacement
-Glucocorticoids or Thyroid or estrogen / testosterone based on underlying deficiency👇🏽
17/

⚡️Primary adrenal insufficiency occurs rarely with ICIs
⬆️ ACTH + ⬇️ cortisol
But if mineralocorticoid-producing cells are affected then metabolic acidosis, ⬇️ BP, ⬆️ K can occur
Rx: Glucocorticoid +/- mineralocorticoids
18/
⬆️ ACTH + ⬇️ cortisol
But if mineralocorticoid-producing cells are affected then metabolic acidosis, ⬇️ BP, ⬆️ K can occur
Rx: Glucocorticoid +/- mineralocorticoids
18/
⚡️ICI-induced diabetes mellitus can occur rarely
Time to onset is highly variable but when it occurs the onset can be rapid therefore it is better to monitor random blood glucose rather than A1C
DKA can occur due to abrupt ⬇️ in insulin
Rx: insulin
19/
Time to onset is highly variable but when it occurs the onset can be rapid therefore it is better to monitor random blood glucose rather than A1C
DKA can occur due to abrupt ⬇️ in insulin
Rx: insulin
19/
⚡️Summary: This table summarizes the Screening, Testing and Treatment of ICI-induced endocrinopathies👇🏽
20/
20/

💥Summary:
⚡️Immune checkpoint inhibitors have transformed cancer Rx
⚡️ICIs can cause auto-inflammation, ⬇️ self-tolerance -> immune-related adverse events
⚡️ICI-induced endocrinopathies can affect the thyroid, pituitary, adrenal & pancreas glands
End/
⚡️Immune checkpoint inhibitors have transformed cancer Rx
⚡️ICIs can cause auto-inflammation, ⬇️ self-tolerance -> immune-related adverse events
⚡️ICI-induced endocrinopathies can affect the thyroid, pituitary, adrenal & pancreas glands
End/
• • •
Missing some Tweet in this thread? You can try to
force a refresh


















