#POCUS #echofirst #MedEd case of the day.
Context: alcoholic liver cirrhosis with suspected #hepatorenal syndrome
Purpose: think about the underlying pathophysiology & seek expert input
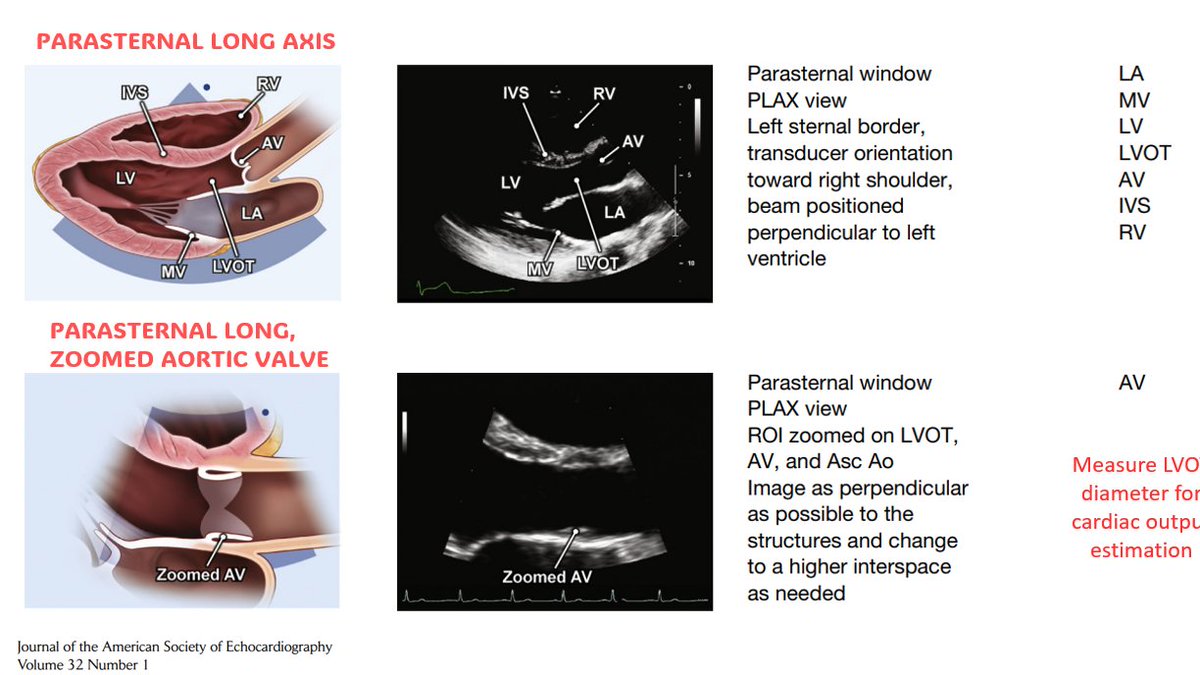
1/ PLAX, PSAX, Apical views of the heart. Heart rate ~110-116 bpm
#VExUS images in 🧵
Context: alcoholic liver cirrhosis with suspected #hepatorenal syndrome
Purpose: think about the underlying pathophysiology & seek expert input
1/ PLAX, PSAX, Apical views of the heart. Heart rate ~110-116 bpm
#VExUS images in 🧵
2/ overall, looks hyperdynamic. LA looks little enlarged on PLAX, visual TAPSE high on apical.
In cirrhosis, hyperdynamic circulation is expected because of splanchnic vasodilatation and 'relative' arterial under filling.
LV EF #POCUS obtained using @kosmosplatform 👇
In cirrhosis, hyperdynamic circulation is expected because of splanchnic vasodilatation and 'relative' arterial under filling.
LV EF #POCUS obtained using @kosmosplatform 👇


4/ Another reading...also LVOT diameter in PLAX = 2.29 cm
With these numbers, LVOT area would be ~4.15 m2
Stroke volume = 115 ml
CO = ~13 L 😳taking heart rate as 110 bpm
With these numbers, LVOT area would be ~4.15 m2
Stroke volume = 115 ml
CO = ~13 L 😳taking heart rate as 110 bpm

5/ Tricuspid tissue Doppler
High S'/Tricuspid annular plane systolic velocity (TAPSV). In general, TAPSV less than 10 cm/sec is said to indicate low RV ejection fraction.
High S'/Tricuspid annular plane systolic velocity (TAPSV). In general, TAPSV less than 10 cm/sec is said to indicate low RV ejection fraction.


7/ Mitral annular tissue Doppler #POCUS:
Lateral e' as high as 20 cm/s
With E-A fusion, is it still possible to say LA filling pressures are normal based on E/e'? experts?
Lateral e' as high as 20 cm/s
With E-A fusion, is it still possible to say LA filling pressures are normal based on E/e'? experts?

8/ Also did RVOT VTI. Just to practice the technique. I understand minor errors in outflow tract diameter lead to significant discrepancy in volume estimation.
VTI ~18 cm, d = 3.1 cm; estimated CO = 14.9 L 😳
Irrespective of error, we can now definitely say its high output state.
VTI ~18 cm, d = 3.1 cm; estimated CO = 14.9 L 😳
Irrespective of error, we can now definitely say its high output state.

9/ How about downstream? IVC #POCUS was difficult to visualize due to abdominal distension. On lateral approach, it appears to be small.
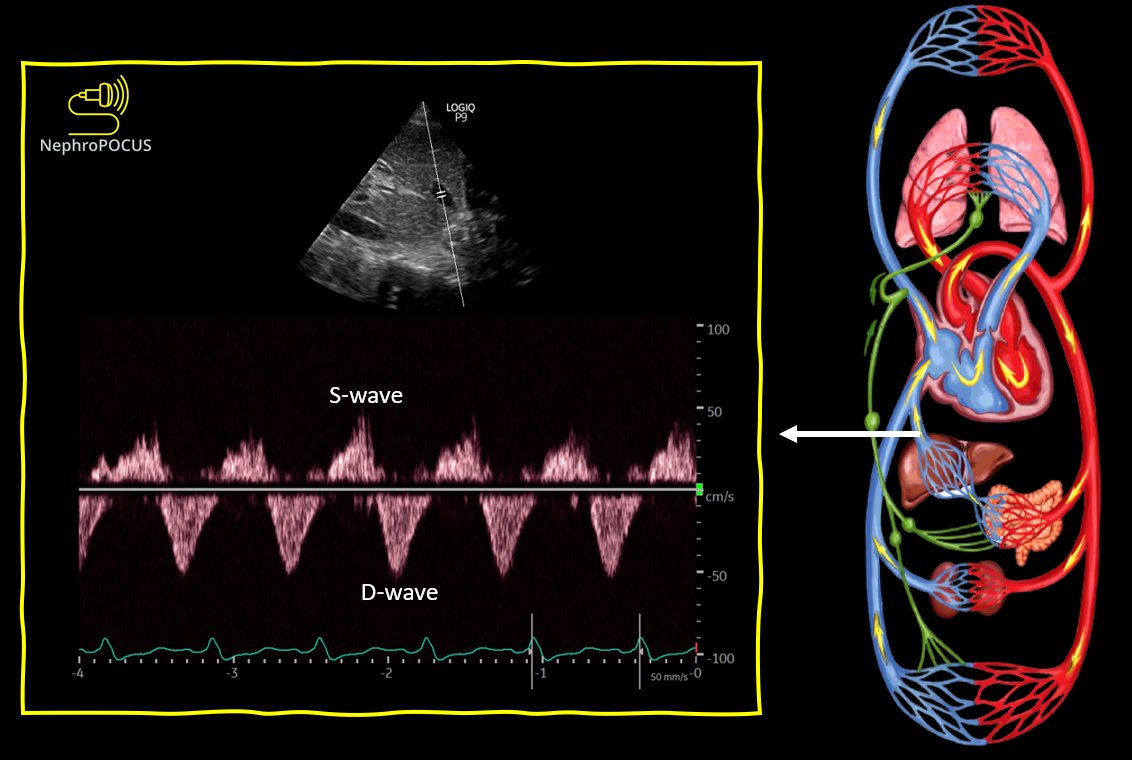
10/ Hepatic color #VExUS

14/ Renal resistive index ~0.74
Difficult to comment if its elevated or not. If you take normal as <0.7, maybe elevated. Its a soft call! #POCUS
Difficult to comment if its elevated or not. If you take normal as <0.7, maybe elevated. Its a soft call! #POCUS

15/ Renal parenchymal vein #VExUS
Normal. Unlikely raised intra-abdominal pressure leading to small IVC
Normal. Unlikely raised intra-abdominal pressure leading to small IVC

16/ Lungs show scattered B-lines with spared areas. Patient had COVID-19 last year. Could be residual changes.
OK, now questions for experts. In this patient with ⬆️serum creatinine, what would you do & what is the rationale?
OK, now questions for experts. In this patient with ⬆️serum creatinine, what would you do & what is the rationale?
17/ Albumin? (CO is already very high), octerotide/midodrine? (BP 118/64 at the time of scan) - what's the goal? or transfer to ICU & give Norepinephrine/Terlipressin?
Likely has a component of cholemic/bile case nephropathy (ATN) also based on urine microscopy.
Likely has a component of cholemic/bile case nephropathy (ATN) also based on urine microscopy.
18/ Also, how would you distinguish chronic hepatorenal pathophysiology from HRS contributing to renal injury (based on ⬆️ #POCUS findings)?
Tagging hemodynamic experts @khaycock2 @ThinkingCC @MDBeni @load_dependent @Thind888 @siddharth_dugar @ArgaizR @iceman_ex @Wilkinsonjonny
Tagging hemodynamic experts @khaycock2 @ThinkingCC @MDBeni @load_dependent @Thind888 @siddharth_dugar @ArgaizR @iceman_ex @Wilkinsonjonny
Cc HRS guru @RegnerKR_Neph for input from #nephrology standpoint.
@threadreaderapp unroll
• • •
Missing some Tweet in this thread? You can try to
force a refresh