1/ Welcome back to #TweetorialTuesday with the #MedEdTwagTeam!
Today begins our series on #EffectiveQuestions in the Clinical Learning Environment.
It’s an age-old practice that can conjure mixed emotions. This series will give you tools to use questions with purpose.
Today begins our series on #EffectiveQuestions in the Clinical Learning Environment.
It’s an age-old practice that can conjure mixed emotions. This series will give you tools to use questions with purpose.

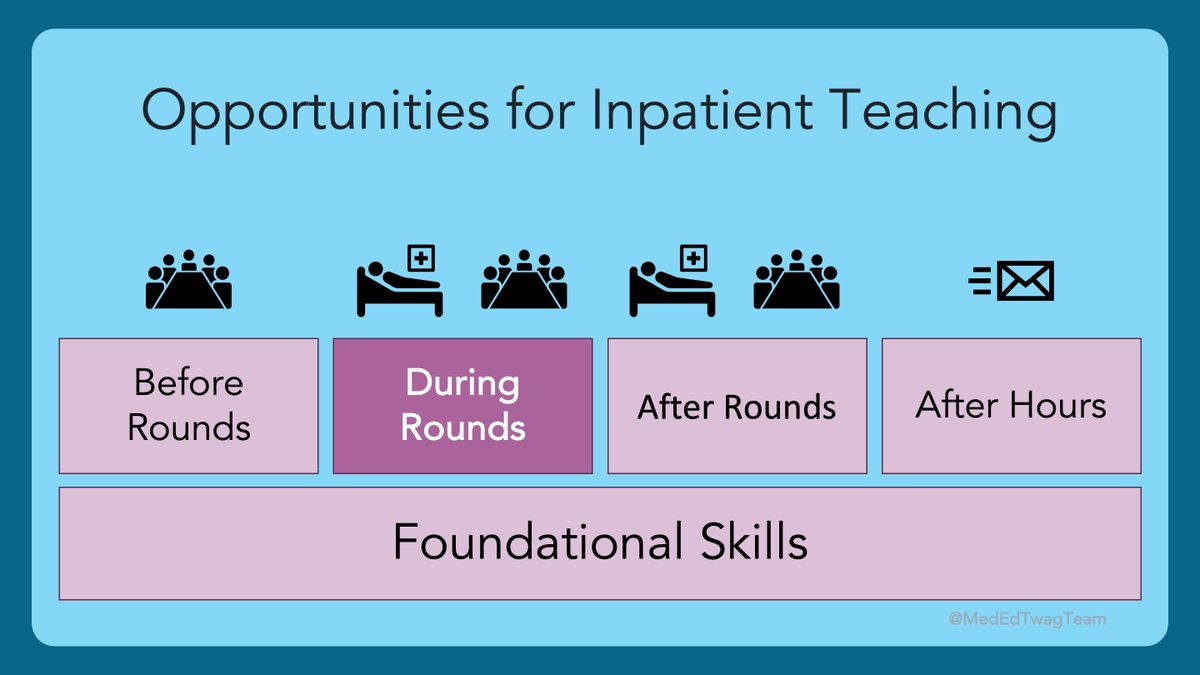
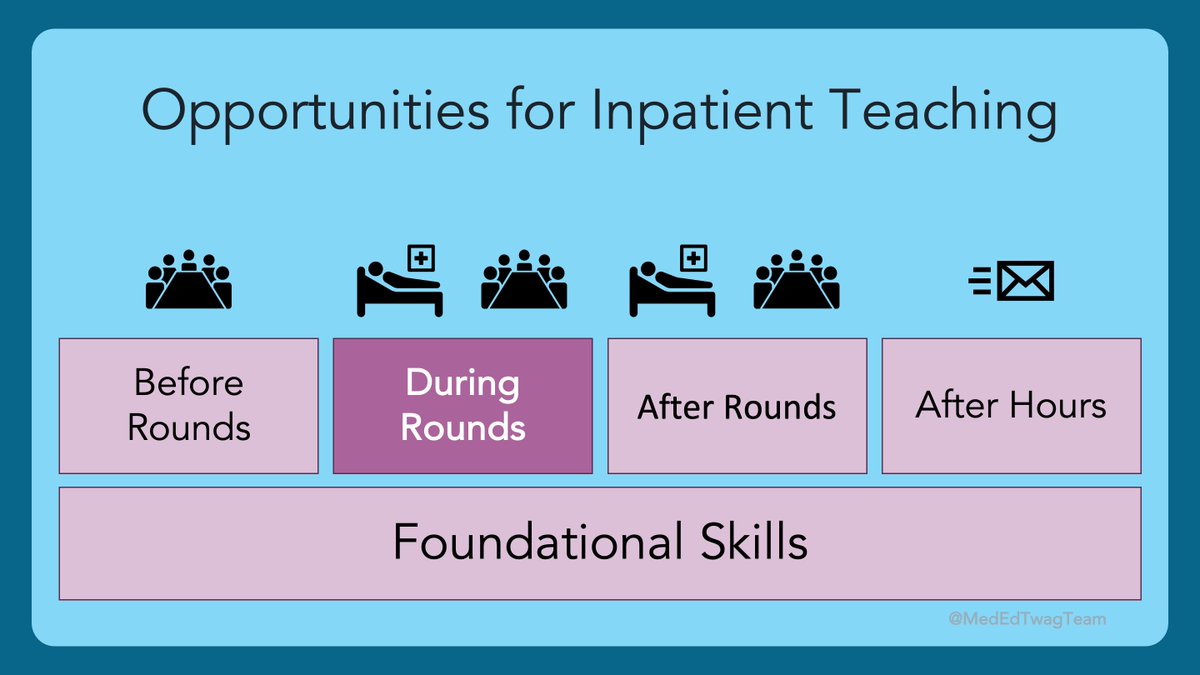
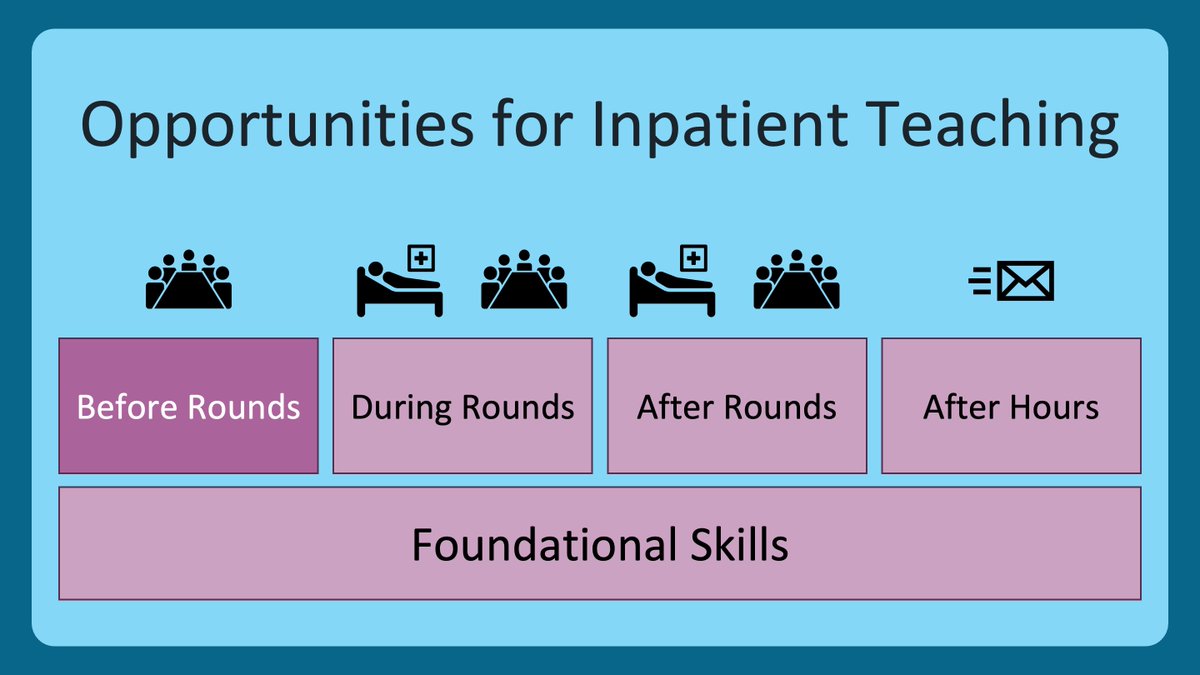
2/ I wanted to bring us back to the #HierarchyOfTeachingSkills that we have been using.
We previously covered the foundational skills that help create psychological safety & we just wrapped up our feedback series.
To see any of these previous threads, check out @MedEdTwagTeam.
We previously covered the foundational skills that help create psychological safety & we just wrapped up our feedback series.
To see any of these previous threads, check out @MedEdTwagTeam.

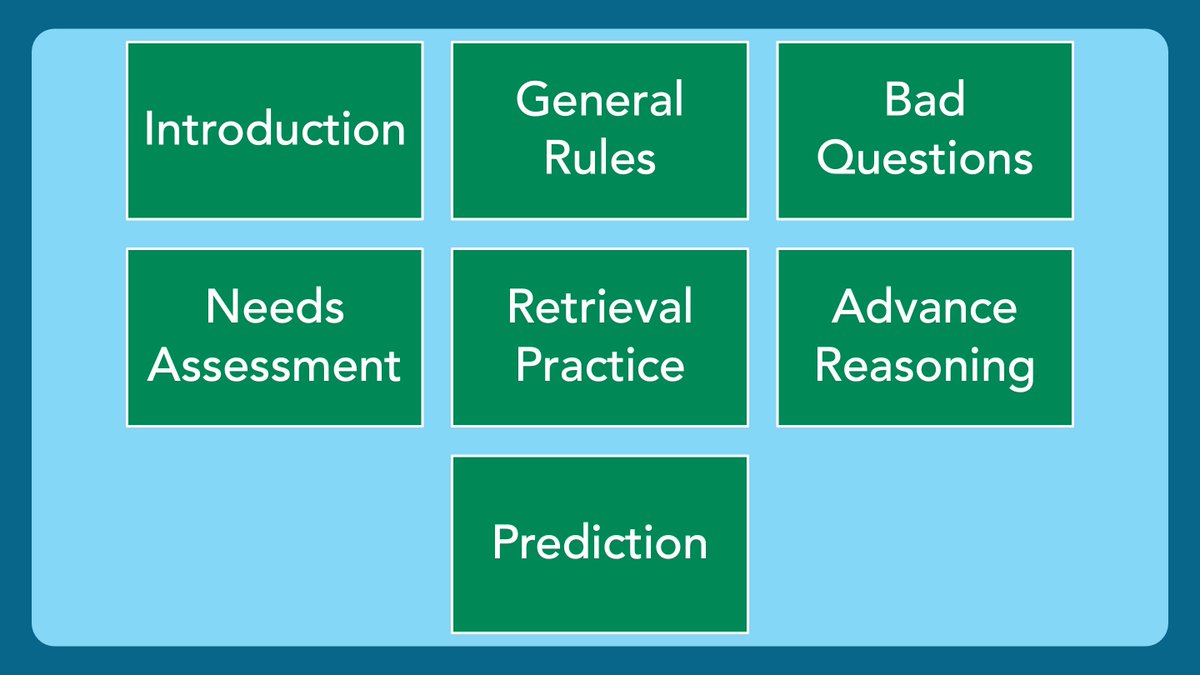
3/ Here is where we are going over the next 7 weeks. Today is our intro.
This is one of my favorite topics in #MedEd!
Questions in the clinical setting are employed by all teachers & SEEM so simple to use.
However, effective questioning is a nuanced skill.
Let’s get into it!
This is one of my favorite topics in #MedEd!
Questions in the clinical setting are employed by all teachers & SEEM so simple to use.
However, effective questioning is a nuanced skill.
Let’s get into it!

4/ Questions, when used improperly, have the potential to cause learners to experience some serious psychological danger (opposite of safety).
Check out this fascinating study in which @egoebs asked pathology residents to draw a “pimping” encounter.
pubmed.ncbi.nlm.nih.gov/31084222/
Check out this fascinating study in which @egoebs asked pathology residents to draw a “pimping” encounter.
pubmed.ncbi.nlm.nih.gov/31084222/

5/ The previous slide introduces the term “pimping”.
There has been much debate, but we agree with the authors of this paper, that the term itself is problematic, & the idea of using questions to humiliate or establish hierarchy is appalling.
pubmed.ncbi.nlm.nih.gov/25099239/
There has been much debate, but we agree with the authors of this paper, that the term itself is problematic, & the idea of using questions to humiliate or establish hierarchy is appalling.
pubmed.ncbi.nlm.nih.gov/25099239/

6/ Today, we won’t get into the content, because I want to hear from you!
I would love to highlight some of your collective wisdom and experiences in the upcoming threads. Don’t be shy!
I would love to highlight some of your collective wisdom and experiences in the upcoming threads. Don’t be shy!
7/ TRAINEES (students, residents, fellows)! Reply with your thoughts to these ?s:
OF NOTE:
A “good question” is: one you think is fair and can lead to learning on your part.
A “bad question” is: one you think is UNfair and/or has little learning value.
OF NOTE:
A “good question” is: one you think is fair and can lead to learning on your part.
A “bad question” is: one you think is UNfair and/or has little learning value.

8/ TEACHERS (residents, fellows, attendings)! Reply with your thoughts to these ?s:
OF NOTE:
A “good question” is: a question you think is fair and can lead to learning for trainees.
A “bad question” is: a question you think is UNfair and/or has little learning value.
OF NOTE:
A “good question” is: a question you think is fair and can lead to learning for trainees.
A “bad question” is: a question you think is UNfair and/or has little learning value.

9/ Alright my #MedTwitter, #MedEd, #MedStudentTwitter friends! I can’t wait to learn from you all!
We will see you back here next week to talk about general rules for asking #EffectiveQuestions in the clinical learning environment.
See you then!
We will see you back here next week to talk about general rules for asking #EffectiveQuestions in the clinical learning environment.
See you then!

• • •
Missing some Tweet in this thread? You can try to
force a refresh