
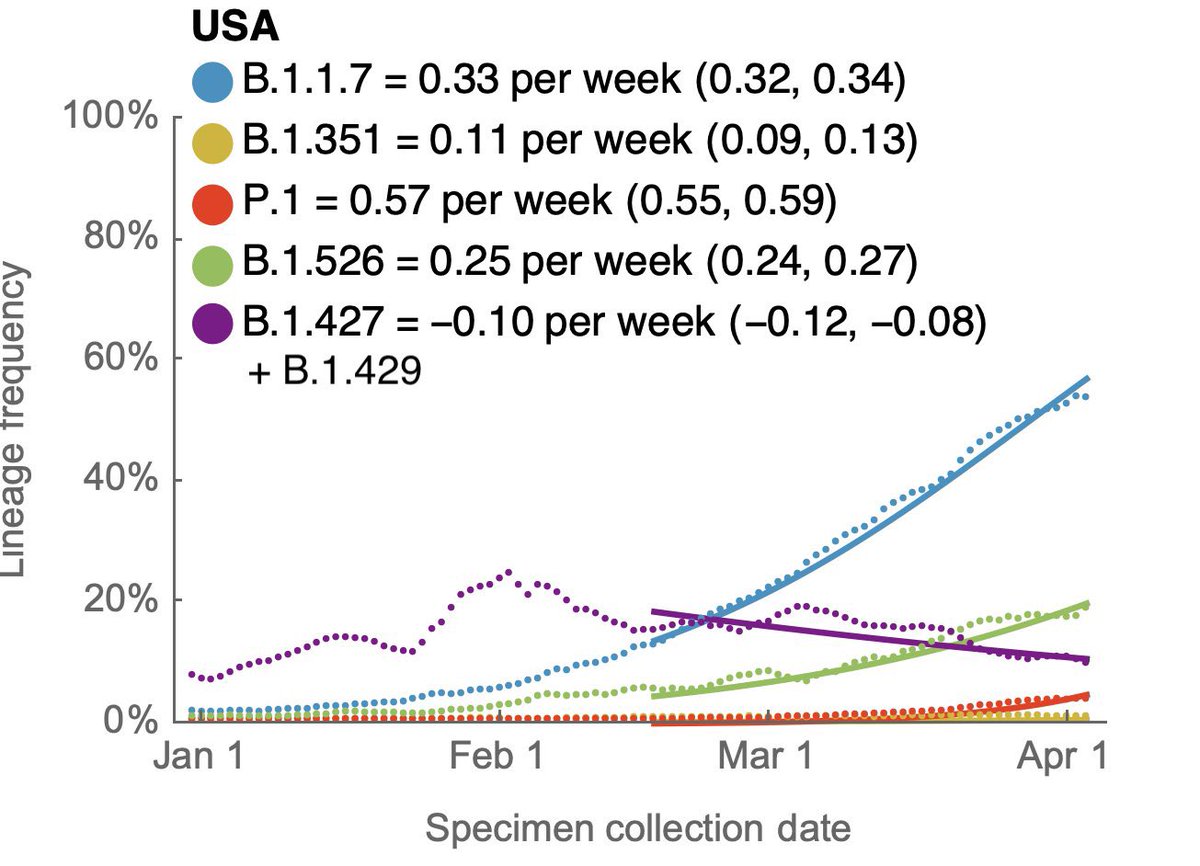
What is the fastest growing variant in the US currently? Not #B117 anymore (now #2)—it’s actually the #P1 variant from Brazil 🇧🇷.
So @NYCHealthCommr Dr @davechokshi is indeed correct when he rightfully pointed out #P1 is “growing” in New York City. #COVID19
(Figure from @trvrb)
So @NYCHealthCommr Dr @davechokshi is indeed correct when he rightfully pointed out #P1 is “growing” in New York City. #COVID19
(Figure from @trvrb)

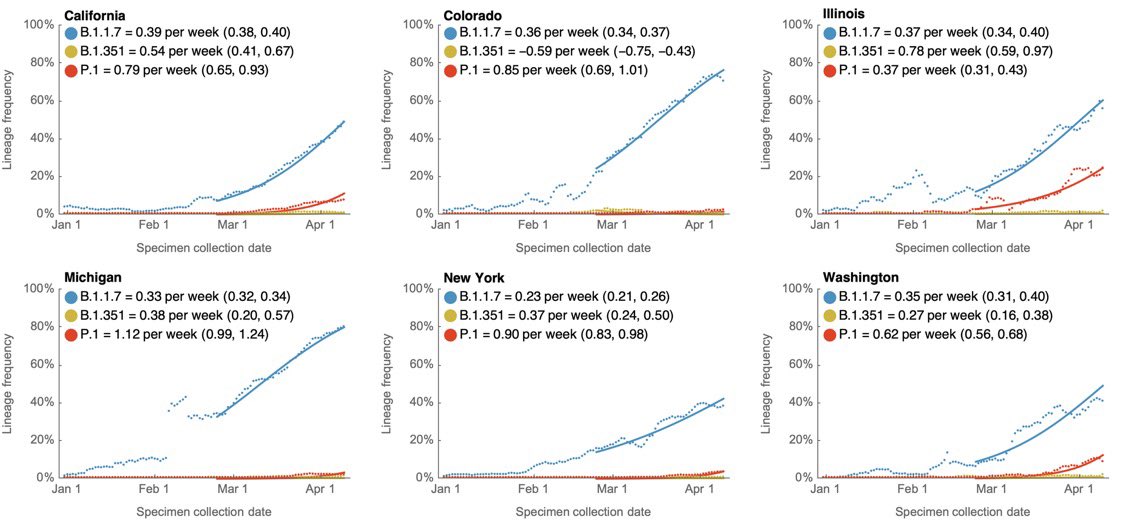
2) In these states, #P1 variant is rising as fast or faster than even #B117. Look at Illinois especially, #P1 is now over 30% of all cases suddenly.
Most of these places as well vaccinated as NYC. Yet #P1 still growing.
Most of these places as well vaccinated as NYC. Yet #P1 still growing.
https://twitter.com/trvrb/status/1388286671267921922
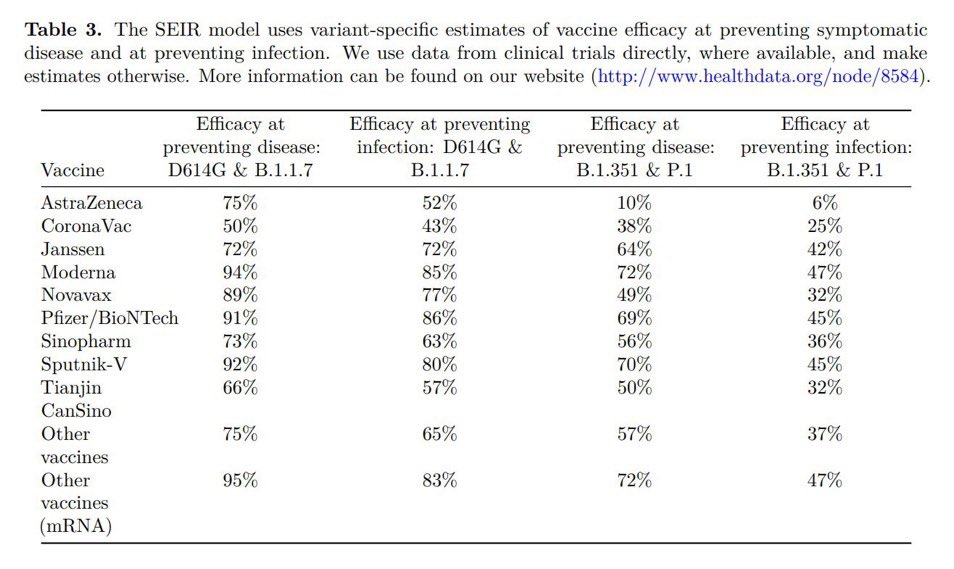
3) Why so I worry about the #P1 variant so much? Because this is the estimated approximate efficacy against transmission by the major vaccines, according to @AliHMokdad of the renowned @IHME_UW epidemiology institute.
Zoom in—right column.
Zoom in—right column.
4) I also deeply worry about #P1 because I’ve seen what happened with #P1 in British Columbia 🇨🇦 last month after they ignored it. It was a complete cluster.
https://twitter.com/drericding/status/1382181545709027331
5) Yes #P1 started incredibly slow at the beginning. Didn’t look that alarming… yet we know how it ended.
https://twitter.com/drericding/status/1374855382200414208
6) Here is a better table of estimated vaccine efficacy from @IHME_UW’s @AliHMokdad — the colored boxes are estimated.
source: healthdata.org/node/8584
source: healthdata.org/node/8584

7) Here is the modeled growth of the #P1 (green) variant from Brazil 🇧🇷 in Belgium 🇧🇪.
Very similar to many other places.
Very similar to many other places.

8) Here is also Washington state (bordering the #P1 hotspot of BC Canada 🇨🇦)… #P1 is also growing. P1 is now 9.7% of all sequenced samples.
https://twitter.com/mel4justice/status/1387982229477855234
• • •
Missing some Tweet in this thread? You can try to
force a refresh




















