
Reflecting how my journey on PDA, has gone from "rebranded autism" in 2017, next a pseudo syndrome resulting from interaction of autism & various comorbids. To it is a common Disorder.
Anyone want to take bets, I will view it as a rare autism subtype (joke)?
Anyone want to take bets, I will view it as a rare autism subtype (joke)?
I should point, I can see why people think PDA is rebranded autism/ a pseudo syndrome resulting from interaction of autism and various comorbids.
I can see why people think PDA is a rare autism subtype. I think that outlook is not cogent, nor particularly scientific nor ethical. I can go into detail why I hold that view. 




Although, I suspect some would argue it is cognitive dissonance with PDA. I cannot accept the demand that PDA is autism. I am being dogmatic & narrow minded calling for scientific-method-based approach to PDA, maintaining integrity of autism.
I need to reflect upon this more.
Tangent, but I am making this a generic thread on more reflections on PDA.
https://twitter.com/Richard_Autism/status/1392401487855243264
I am also pretty certain, I can explain the weird academic decisions in PDA literature, by assuming that their is an agenda to view PDA as an ASD; probably out of genuine (mistaken) belief PDA is autism.
I am talking about weird things like repeatedly missing/ ignoring non-autistic persons in PDA samples. Likewise, Newson's views on the topic, how she excluded those with autism features from her cohort & NOT basing PDA on the Triad of Impairment etc etc.
It based on the view that it is an axiom that PDA is an ASD, so it is taken as a truth that PDA is autism. We know that there was a research agenda proposed that PDA is an ASD in 2011. That they approached PDA as an ASD.
repository.tavistockandportman.ac.uk/2165/
repository.tavistockandportman.ac.uk/2165/

This process is the same one that lead to Newson viewing PDA as having Coding issues, which is when a person struggles to understand/ process certain aspects of communication.
Newson created her own diagnostic grouping called "Pervasive Developmental Coding Disorders" & used it between 1986 - 1996. She created the diagnostic grouping, before she created PDA's behaviour profile in 1988.
We know that Newson was questioning what Coding issues PDA had in 1986, see the diagram below. Newson needed PDA to have Coding issues to fit into her newly created diagnostic grouping.

Newson was aware she was reifying PDA when she created her behaviour profile in 1988.
Newson's decision to assume PDA was a Pervasive Developmental Coding Disorder, explains why her behaviour profile has one social communication issues trait of: "Surface sociability, but lack of sense of identity, pride, or shame."
We also know that specific trait is highly problematic. Much of its features are either RRBIs in nature, i.e. not social communication issues. Or, do not reliably measure its proposed deficits in social identity/ pride/ shame.

We also know that PDA is not meant to have Theory of Mind deficits and this is supported by Bishop (2018). There are many good reasons to be skeptical of viewing PDA as having Coding issues.

So, what do I think is happening with weird academic decisions in PDA literature, around viewing PDA as an ASD. Is the same processes, is that such decisions are derived from the need that to have PDA as an ASD.
One cannot assume and treat PDA as an ASD, if one acknowledges their are non-autistic persons with PDA in various research samples. Likewise, PDA is not based on triad of impairment. Or, not caused by autism. Etc etc.




I unsure of how much of this academic "silliness" is deliberate or not. We know generally, PDA is an ASD supporters do not engage with critique & do not reference divergent literature. Similarly, generally aggressively lobbying for PDA to be viewed as an ASD.
The decision to view PDA as an ASD, does seem to be deliberate though. That there are substantial conflicts of interests present in how it is being portrayed and pursued.
One big difference between me and "PDA is an ASD" supporters, generally, is that I am open I have a conflict of interest in advocating for PDA to be viewed as a common Disorder & it should be practiced as such.
I am still reflecting on the initial tweets in this thread. How much of my views are driven by cognitive dissonance or not? Am I being narrow minded/ dogmatic? Am I being unreasonable or not?
I am being dogmatic calling for good quality ethics and practiced around PDA, i.e. scientific-method and inclusive based approach to PDA. I only see that insistence as a positive thing. Quality of ethics & research are often mutually interacting.
I, like all autism stakeholders, should be striving to raise the poor quality standards, of much autism research, policy and practice (which PDA is unfortunately being associated with autism).
Generally, I think I am being incredibly open minded on PDA. Also highly creative in my approach and rationale about it. I am open to exploring logic, to see where it leads to.
I am still reflecting on. if my rationale on me being open minded etc is strong and robust. I am also wondering if I am just pointless doubting myself. Sometimes it is beneficial to question oneself and ones own biases and assumptions.
To me, this is all part of being a responsible researcher, to critically engage with things and to reflect on things.
I am autistic, a highly intelligent person, who is obsessed with PDA. I naturally reflect about it by default, like making a cup of tea etc.
I am autistic, a highly intelligent person, who is obsessed with PDA. I naturally reflect about it by default, like making a cup of tea etc.
To underline the point in this tweet, if one is critically reflecting on PDA, noticing MANY/ ALL the reasons PDA is NOT autism; logical thing to do is assume PDA is NOT autism. Which is what happened to me about 18 months ago.
https://twitter.com/Richard_Autism/status/1392410233897693184
The point is, that it becomes absurd to view PDA is an ASD, when there are like two dozen/ plus reasons PDA is not an ASD. There are substantial more reasons to NOT view PDA as an ASD, when compared to 18 months ago.
From my understanding there is a strong case PDA is not autism; which is essentially why I hold that position.
I have put more reasons in the slides why it is problematic viewing PDA as having Coding issues. Now across three slides.
Tangent, I thinking of using widescreen slides in the future, so may well be on less slides in the future.
Tangent, I thinking of using widescreen slides in the future, so may well be on less slides in the future.



I have been reflecting on the problems with proposed coding issues in PDA. Blog post by Donna Williams is important, as it explains rationale behind proposed deficits in social identity/ pride/ shame. I have updated the slides again. blog.donnawilliams.net/2008/06/17/exp…




The being highly motivated and avoiding demands by choice, with it being viewed as a psychological in nature explains why most PDA tools have items with behaviours done with intent behind them.
I can see why some might say, I am being rigid on PDA, by not viewing it as an ASD. I would point to the strong case, WHY PDA is not an ASD, and the examples about me being open minded on it.
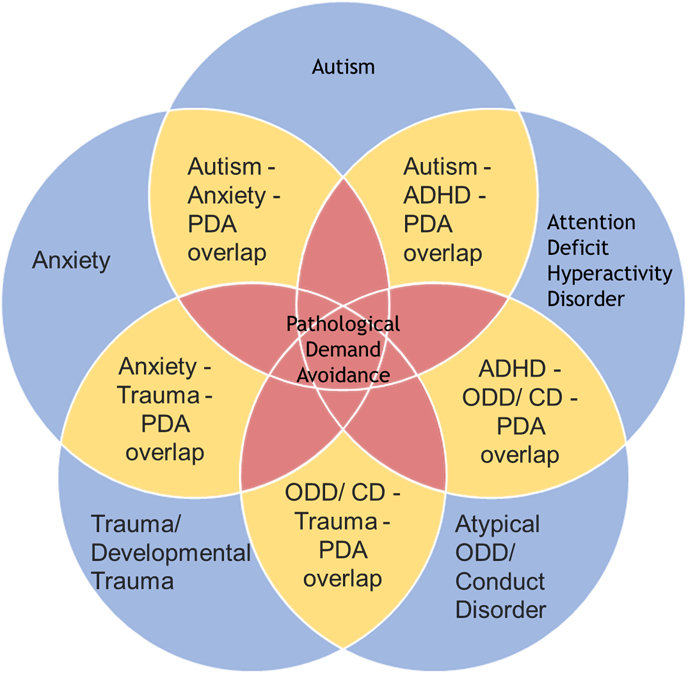
Example, my edited version of Soppitt, 2021, p299, diagram of how PDA relates to other conditions.

My version of the diagram, I added anxiety to it, to reflect certain research results. In my view I would personally remove autism from it, but in order to reflect some research results, autism should be included.
Example of how I conceptualise PDA vs DSM-5 autism, is here. First image is from Rosen et al (2021). Second image is my one, mapping PDA features relative to Rosen et al (2021) image.
PDA features should hallow DSM-5 autism criteria.
link.springer.com/article/10.100…
PDA features should hallow DSM-5 autism criteria.
link.springer.com/article/10.100…


I would also add, it is large journey that has came about from much reflection reading on PDA, to go from rebranded autism:
tandfonline.com/doi/full/10.10…
tandfonline.com/doi/full/10.10…
To PDA is a pseudosyndrome to resulting from interaction of autism and various co-occurring conditions:
researchgate.net/publication/33…
researchgate.net/publication/33…
Through to current position of PDA probably is a new type of common Disorder:
thepsychologist.bps.org.uk/pda-new-type-d….
thepsychologist.bps.org.uk/pda-new-type-d….
If you compare this to journey to some prominent PDA is an ASD supporters, it is very striking the difference path to present positions.
Take Christie 2007, that PDA was needed to replace many persons who received a PDD-NOS diagnosis (I am unsure if Christie understood Newson's PDD-NOS is not the same as the DSM-4 one though).
ingentaconnect.com/contentone/bil…
ingentaconnect.com/contentone/bil…

Newson's PDD-NOS includes those not meeting clinical threshold for either: Autism/ Asperger's Syndrome/ PDA/ Specific Language Impairments (including dyslexia & dysphasia). So includes many non-autistic persons.

DSM-4 PDD-NOS, is for those not meeting threshold for either Asperger's/ Autistic Disorder. PDD-NOS in this view is an ASD subtype.
Newson's PDD-NOS is not an autism subtype.
adc.bmj.com/content/88/7/5…
Newson's PDD-NOS is not an autism subtype.
adc.bmj.com/content/88/7/5…


The starting position of Newson's work, is that PDA is relatively common & seen in non-autistic persons. This is reflected in Christie's article, not all of Newson's cohort would have received a diagnosis of a DSM-4 autism subtype.


Since then, there has been research that viewed PDA to be a rare autism subtype, using an arbitrary threshold of 30% or less for PDA traits.
Guess who who was a co-author to the paper (rhetorical)?
link.springer.com/article/10.100…
Guess who who was a co-author to the paper (rhetorical)?
link.springer.com/article/10.100…


An important to point consider here, is that this research went out of their way to view PDA as an ASD subgroup. This contradicts Newson's approach to PDA.
adc.bmj.com/content/archdi…
adc.bmj.com/content/archdi…



"Clearly, “hanging together as an entity” is not enough if that entity is not significantly different from both autism and Asperger’s syndrome, either separately or apart" (Newson et al, 2003, p599).
Point is Newson, is trying to make PDA an Autism subtype/ profile/ subgroup (anything part of the autism spectrum). She is trying to justify PDA is clinically needed because it is different & therefore not autism.
Must also be said, it seems Newson appreciated her PDD-NOS does not conform to accepted DSM-4 PDD-NOS and accepted "autism spectrum", as she viewed "autistic spectrum" to only consist of Asperger's & Kanner's autism.

Where am I going with this, simple answer, more recent even narrower PDA definitions, adopted by a PDA is an ASD diagnosing clinic.
I set out here, these definitions are incredibly narrow, compared to other PDA diagnostic thresholds.
rationaldemandavoidance.com/2021/04/25/pda…
I set out here, these definitions are incredibly narrow, compared to other PDA diagnostic thresholds.
rationaldemandavoidance.com/2021/04/25/pda…

So, what we have had from prominent PDA is an ASD supporters, is a progressive narrowing of PDA, from Newson's to what I refer to as "Extreme Extreme Demand Avoidance".


Bare in my mind my previously posted blog post has been described as:
“having done an absolutely first class job of summarising all the past literature and perspectives on PDA. No one else has done anywhere near as good, or as thorough, a job as you have.”
“having done an absolutely first class job of summarising all the past literature and perspectives on PDA. No one else has done anywhere near as good, or as thorough, a job as you have.”
Reasons why I call this narrowly defined PDA as "Extreme Extreme Demand Avoidance", can be found here:
threadreaderapp.com/thread/1391308…
threadreaderapp.com/thread/1391308…
Where am I going with this. It seems inherently problematic to view me as being dogmatic/ closed minded on PDA, when I have progressively evolved my view in open minded manners, while others have adopted narrower/ rigid interpretations on PDA.
I will end this thread here.
@threadreaderapp please could you do your thing (unroll these tweets)?
Thank you in advance.
@threadreaderapp please could you do your thing (unroll these tweets)?
Thank you in advance.
I need to point out that Newson was NOT trying to make PDA autism, if anything she seems to make a concerted effort to make PDA NOT autism. We know she viewed PDA to NOT be autism over at least a 20 year time period.
@threadreaderapp Please could you unroll?
• • •
Missing some Tweet in this thread? You can try to
force a refresh





