
Acute Kidney Failure
OR 🤔
Acute Kidney Success?
…bare with me while I explain 🧵
#NephTwitter #MedTwitter #Physiology #askrenal #tweetorial #aki #MedStudentTwitter #meded #FOAMed
OR 🤔
Acute Kidney Success?
…bare with me while I explain 🧵
#NephTwitter #MedTwitter #Physiology #askrenal #tweetorial #aki #MedStudentTwitter #meded #FOAMed
We make 1-2 L of urine per day to eliminate
❎excess solutes
❎H2O
❎toxins
AND
✅maintain homeostasis.
This process is accurate to the T.
❎excess solutes
❎H2O
❎toxins
AND
✅maintain homeostasis.
This process is accurate to the T.
To achieve this accuracy, plasma is continuously filtered and reprocessed by the kidneys. ♻️
How much plasma is filtered per day, you ask? 😳
Roughly 200 LITRES! 🌊
How much plasma is filtered per day, you ask? 😳
Roughly 200 LITRES! 🌊

Yes, that’s correct.
8L of plasma is filtered, processed, and reabsorbed by the kidney every HOUR 💦
Gist? The ENTIRE plasma volume is filtered and reabsorbed TWICE an HOUR🤯
8L of plasma is filtered, processed, and reabsorbed by the kidney every HOUR 💦
Gist? The ENTIRE plasma volume is filtered and reabsorbed TWICE an HOUR🤯
🔅The glomerulus filters.
🔅The tubules reabsorb.
So?
If the kidney looses TUBULAR function (hint hint.. as in ATN…), and reabsorption ceases, the entire plasma volume will be lost in less than an hour❗️
Hence, tubular injury should NOT be compatible with LIFE.
🔅The tubules reabsorb.
So?
If the kidney looses TUBULAR function (hint hint.. as in ATN…), and reabsorption ceases, the entire plasma volume will be lost in less than an hour❗️
Hence, tubular injury should NOT be compatible with LIFE.
...last I checked, we were not inserting cordis catheters to resuscitate AKI patients with 8L of IVF per hour 🧐
...patients with acute kidney injury do not succumb within an hour to a devastating loss of plasma volume 💀
To the contrary, urine volume DECREASES (oliguria).
...patients with acute kidney injury do not succumb within an hour to a devastating loss of plasma volume 💀
To the contrary, urine volume DECREASES (oliguria).
Glomerular filtration is powered by the left ventricle. 🫀
Tubular reabsorption is powered by ATP and defines the composition of both the plasma and the filtrate. ⚖️
However, they do NOT work independently of each other… they talk 🗣
Tubular reabsorption is powered by ATP and defines the composition of both the plasma and the filtrate. ⚖️
However, they do NOT work independently of each other… they talk 🗣
… here comes the beautifully orchestrated link.
The glomerulus and the distal convoluted tubule kiss to form the tubuloglomerular feedback - an adaptive mechanism that allows adjustment of filtration rate to the reabsorptive capacity of the tubules
The glomerulus and the distal convoluted tubule kiss to form the tubuloglomerular feedback - an adaptive mechanism that allows adjustment of filtration rate to the reabsorptive capacity of the tubules
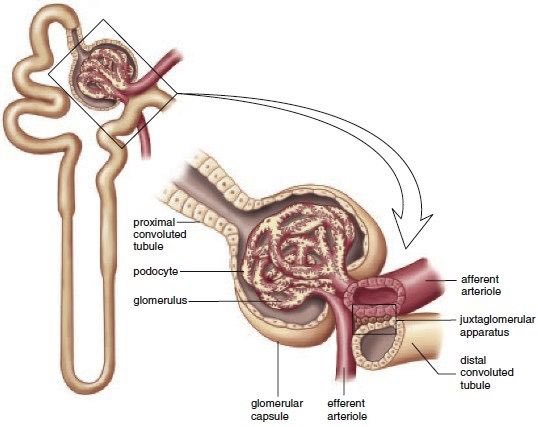
While in intimate apposition, cells of the distal tubule (differentiated here into macula dense cells), communicate with the vascular pole of the glomerulus
Juxtaglomerular apparatus
Macula densa cells are packed with RENIN and sense the Cl content of the distal tubule fluid
Juxtaglomerular apparatus
Macula densa cells are packed with RENIN and sense the Cl content of the distal tubule fluid

If the Cl content of the tubular fluid at the distal tubule is HIGH...
...due to the failure of the more proximal segments of the tubules to reabsorb the filtered content...
...RENIN activity increases and angiotensin II is formed locally/intrarenally.
...due to the failure of the more proximal segments of the tubules to reabsorb the filtered content...
...RENIN activity increases and angiotensin II is formed locally/intrarenally.
These hormones immediately reduce GLOMERULAR FILTRATION by vasoconstriction of the glomerular arterioles.
Filtration is reduced to a level compatible with the reduced reabsorptive capacity.
Filtration is reduced to a level compatible with the reduced reabsorptive capacity.
Hence, to conform to the attenuated reabsorptive capacity of the tubules, the glomeruli decrease filtration in parallel.
OLIGURIA ensues - this is SUCCESS.
✅✅✅
OLIGURIA ensues - this is SUCCESS.
✅✅✅
Were the GFR to remain normal while the tubular reabsorptive capacity were reduced by 80%...
...the patient would loose their entire plasma volume within an hour and unless you were to replete 4 to 5 L per hour...
...the serious fluid losses would be lethal.
☠️ 💀
...the patient would loose their entire plasma volume within an hour and unless you were to replete 4 to 5 L per hour...
...the serious fluid losses would be lethal.
☠️ 💀
Next time, you see a patient with oliguric renal failure - thank the ever compatible tubule-glomerular relationship!
Otherwise, only emergent nephrectomy could have allowed plasma volume preservation when the tubules failed.
Reversible glomerular shut down is a life saving adaptive response.
Acute renal success.
Reversible glomerular shut down is a life saving adaptive response.
Acute renal success.
• • •
Missing some Tweet in this thread? You can try to
force a refresh


