So Dr. Reddy's has revealed the actual primary end point of their Phase 3 #2DG trial. They claim this was pre-specified and I guess we'll have to take their word 4 it.
But, wait a minute.. what was the +ve outcome they presented to DCGI? Was it time to 2 point improvement? 1/n
But, wait a minute.. what was the +ve outcome they presented to DCGI? Was it time to 2 point improvement? 1/n
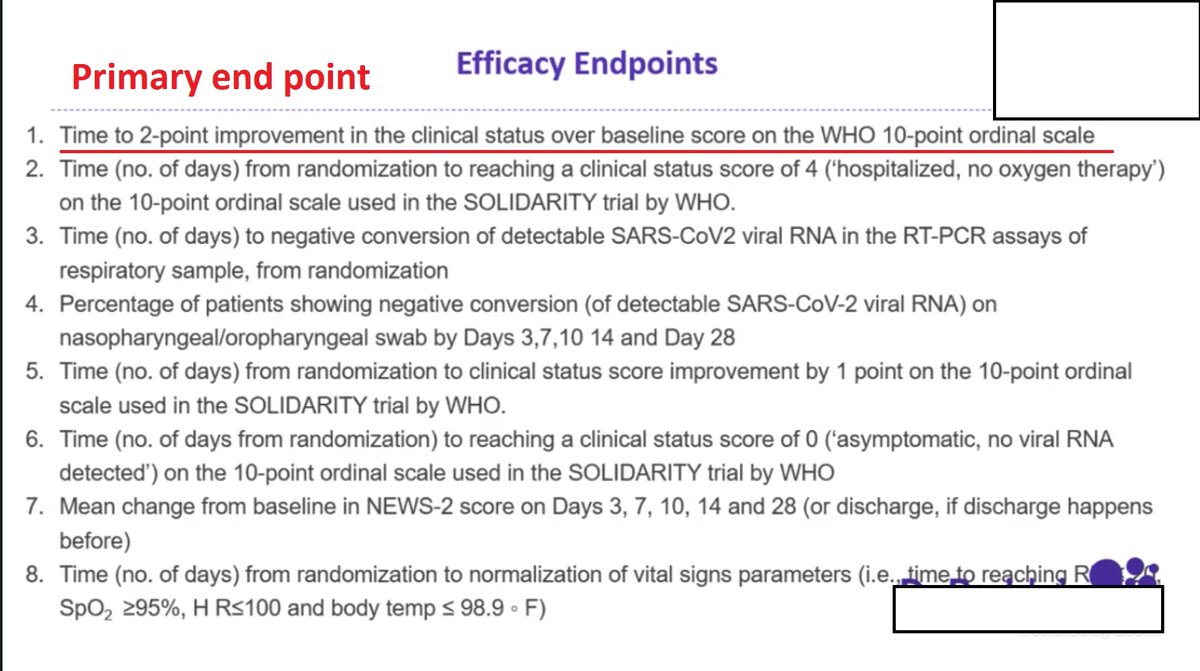
Umm, this sounds very different - they presented only proportion of patients with 1 point improvement at Day 3. Which if u recheck the last tweet, wasn't even one of their secondary end points! 2/n

What happened to all the other endpoints? Time to 2-pt imp, Time to reach pt 4, Time to pt 0, Time to negative PCR? What happened to these patients on Day 5, Day 7, Day 14??
Where is the test for statistical significance? Note that there is ZERO relevance of stating the RRR.. 3/n
Where is the test for statistical significance? Note that there is ZERO relevance of stating the RRR.. 3/n
or the relative risk reduction here. They have not shown survival curves which wld tell us if there was consistent improvement between the arms.
It's very possible that on Day 5 there was no difference at all, and both grps might have had a similar outcome. 4/n
It's very possible that on Day 5 there was no difference at all, and both grps might have had a similar outcome. 4/n
No mention of clinically meaningful outcomes like how many got worse, how many ended up on ventilator, dying, etc. No mention of adverse effects, nothing.
They claim they are still tabulating those. So is this an interim analysis? I hardly think so. 5/n
They claim they are still tabulating those. So is this an interim analysis? I hardly think so. 5/n
Why was adverse event data not submitted to DCGI of the phase 3? Why are they hiding the actual outcome data of their pre-specified outcomes?
My guess: They either lost too many to follow up (as they stated during the slide presentation) and so the data from Day 3 onwards 6/n
My guess: They either lost too many to follow up (as they stated during the slide presentation) and so the data from Day 3 onwards 6/n
is of too few patients for any reasonable analysis, or they didn't like the results they got and they are cherry picking.
I'm saddened that time and again, incomplete, irrelevant, clinically useless and shady results can be presented in a scientific forum and be accepted 7/n
I'm saddened that time and again, incomplete, irrelevant, clinically useless and shady results can be presented in a scientific forum and be accepted 7/n
When did we forget to ask questions?
Why don't we demand better from our drug regulators who are supposed to look out 4 patients and not for the companies?
How many more such underwhelming and probably useless "wonder drugs" will they keep approving 4 people to then spend hrs 8/n
Why don't we demand better from our drug regulators who are supposed to look out 4 patients and not for the companies?
How many more such underwhelming and probably useless "wonder drugs" will they keep approving 4 people to then spend hrs 8/n
searching everywhere for in a desperate attempt to save their loved ones?
Even now, there are so many tweets begging 4 2DG to give a critically ill patient.
THIS DRUG WAS NOT EVEN TRIALLED ON CRITICALLY ILL PATIENTS. 9/n
Even now, there are so many tweets begging 4 2DG to give a critically ill patient.
THIS DRUG WAS NOT EVEN TRIALLED ON CRITICALLY ILL PATIENTS. 9/n
TL; DR: unblinded open label trial of old molecule in moderate Covid which used meaningless soft (manipulatable) end-points, did not even report the results of those end-points, is now being used to advertise a drug as "life saving". This has to be a low point for science! 10/10
@PriyankaPulla @drabbyphilips @ronaklmno @d_s_thakur @ProfSomashekhar @das_seed @VarugheseDeepak @Charakan @sandygrains @GorwayGlobal @pash22 @Neurophysik @abledoc @deralteGaukler @just1doctorwala @DrJoyeeta @pseudo_sapiens @pythoroshan
Linking my original thread explaining what a primary endpoint is and why it shd be prespecified
https://twitter.com/drcheruvarun/status/1391409220667408390?s=19
• • •
Missing some Tweet in this thread? You can try to
force a refresh