
DVT as a feature of #VITT: unusual in the UK / Europe yet common in Australia - could cases have been missed?
NB this is a loose theory, not an assertion
Here are some observations
NB this is a loose theory, not an assertion
Here are some observations
On 20 May ATAGI reported a breakdown of types of clot seen in 🇦🇺 VITT cases
Of 21 confirmed + 3 probable cases, DVT was present in 12 (50%)
Even excl. probables + assuming all 3 included DVT, that would mean DVT present in minimum 9 / 21 = 43% VITT cases
tga.gov.au/periodic/covid…
Of 21 confirmed + 3 probable cases, DVT was present in 12 (50%)
Even excl. probables + assuming all 3 included DVT, that would mean DVT present in minimum 9 / 21 = 43% VITT cases
tga.gov.au/periodic/covid…
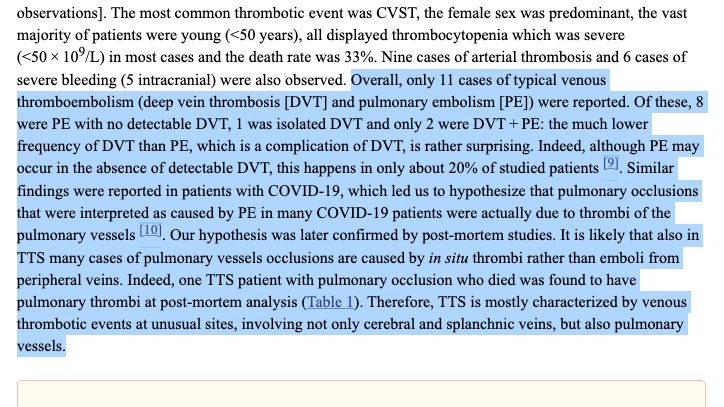
In Europe only 3 / 45 (7%) cases across 4 published papers (Schultz, Greinacher, Scully, Tiede) + 1 unpublished study (Scavone) include DVT according to a paper by M Cattaneo
This is strikingly different from the Australian data - what could explain it?
ncbi.nlm.nih.gov/pmc/articles/P…
This is strikingly different from the Australian data - what could explain it?
ncbi.nlm.nih.gov/pmc/articles/P…

1/ Risk of selection bias in the case series which makes the 45 European cases unrepresentative of VITT cases in Europe generally?
Seems not to be the case, the various papers suggest all patients who met the criteria for VITT were included, none mention excluding cases
Seems not to be the case, the various papers suggest all patients who met the criteria for VITT were included, none mention excluding cases
Cattaneo (a haematology professor) also specifically comments on the low occurrence of DVT in VITT cases, particularly notable in its absence in cases of PE, suggesting most clots in the lungs in VITT form de novo in the pulmonary vessels rather than starting life as DVTs
2/ Could Australia be using a broader definition of VITT, therefore counting cases which are not "real" VITT?
No, Australia only counts as "confirmed" VITT cases which include thrombosis, thrombocytopenia, high D-dimer and test positive for anti-PF4
No, Australia only counts as "confirmed" VITT cases which include thrombosis, thrombocytopenia, high D-dimer and test positive for anti-PF4

3/ Could the difference be down to chance?
DVT was present in at least 43% of 🇦🇺VITT but only 7% of 🇬🇧🇪🇺🇳🇴VITT
The sample sizes are small and np = 3 for the European data meaning the normal approximation cannot be used
However...
DVT was present in at least 43% of 🇦🇺VITT but only 7% of 🇬🇧🇪🇺🇳🇴VITT
The sample sizes are small and np = 3 for the European data meaning the normal approximation cannot be used
However...
... *even if* Europe had seen more DVTs (say, 5 instead of 3 to permit the normal approximation to the binomial) that would mean comparing 43% and 11% which gives a p value of 0.004
This suggests the difference is not due to chance alone (albeit sample sizes are small)
This suggests the difference is not due to chance alone (albeit sample sizes are small)
So what could be going on?
One difference between the 🇦🇺 cases and the European cases is age. Australia limited #AZ to over 50s in early April, meaning most (75%) of its #VITT cases have been in over 50s
In contrast most of the 45 European cases (over 70%) were in under 50s
One difference between the 🇦🇺 cases and the European cases is age. Australia limited #AZ to over 50s in early April, meaning most (75%) of its #VITT cases have been in over 50s
In contrast most of the 45 European cases (over 70%) were in under 50s
Could this mean DVT is more frequent in VITT in older patients and that 🇦🇺 is detecting more VITT cases than in Europe in older patients?
ATAGI suggests that 🇦🇺 is indeed identifying more #VITT cases than in other countries
ATAGI suggests that 🇦🇺 is indeed identifying more #VITT cases than in other countries

This is also supported by the published incidence rates per 100k of 2.6 in under 50s and 1.6 in over 50s in Australia, vs 2 (under 40) and 1 (over 40) in the UK
It is difficult to draw conclusions using relatively small samples, however...
It is difficult to draw conclusions using relatively small samples, however...
It seems plausible #VITT cases have been missed in UK and Europe
Available data suggests DVT within VITT is more common in over 50s, with the low reported frequency of DVT in VITT outside Australia potentially pointing to under-reporting of VITT specifically in older patients
Available data suggests DVT within VITT is more common in over 50s, with the low reported frequency of DVT in VITT outside Australia potentially pointing to under-reporting of VITT specifically in older patients
• • •
Missing some Tweet in this thread? You can try to
force a refresh


