Our newest study of #emergingfungalinfections
Covid-assoc #aspergillosis reportedly occurs in <1/3 ICU patients, but dx is rarely biopsy confirmed
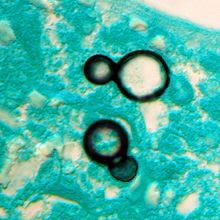
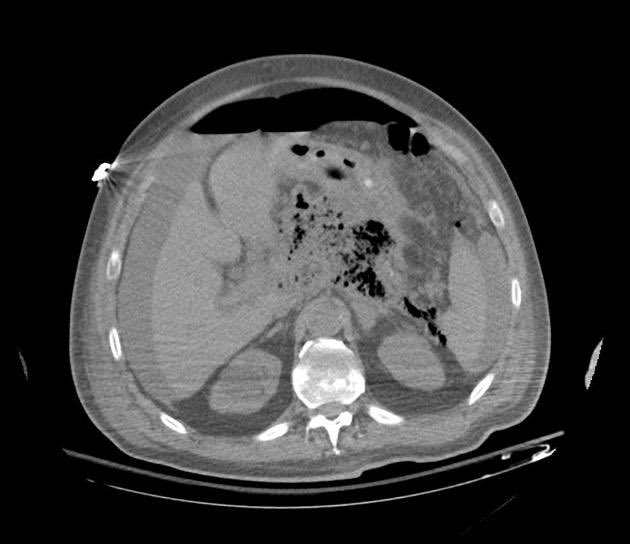
By reviewing autopsy studies, we found proven invasive mould infections occur in 2% of decedents w covid
sciencedirect.com/science/articl…
Covid-assoc #aspergillosis reportedly occurs in <1/3 ICU patients, but dx is rarely biopsy confirmed
By reviewing autopsy studies, we found proven invasive mould infections occur in 2% of decedents w covid
sciencedirect.com/science/articl…




Major caveat is that most autopsies included were from first wave, pre-#RECOVERYtrial and use of steroids and other immunomodulation likely increase risk of #CAPA.
NB to know your local epi, which may differ; for eg of centers reporting >>> rates, see link.springer.com/article/10.100… &👇
NB to know your local epi, which may differ; for eg of centers reporting >>> rates, see link.springer.com/article/10.100… &👇
https://twitter.com/GermHunterMD/status/1407447500860968963
Big congratulations to Dr Brittany Kula (@ScrofKula), ID fellow extraordinaire @UofA_ID and soon @UAlberta_ICU fellow, for doing a wonderful job leading this study. Brittany is pictured in the first tweet, and here is her cat Gladys

Many thanks also to collaborators @ClancyNeil and Hong Nguyen @mhn5pittedu1. This was a companion / complementary study to one Neil led on bacterial superinfections detected on autopsy (which is much more difficult to determine conclusively) academic.oup.com/ofid/article/8…
• • •
Missing some Tweet in this thread? You can try to
force a refresh