
The arrival of new interns in July is an excellent opportunity for us to revisit the basics- today let’s talk about a test that is simultaneously one of the most overused and poorly interpreted tools in medicine: the UA.
Say it with me now… INFLAMMATION ≠ INFECTION
1/10
Say it with me now… INFLAMMATION ≠ INFECTION
1/10
The UA is actually not one test but many! It can roughly be thought of in 3 separate parts: renal, metabolic, and inflammatory panels. Bundling these together can lead to diagnostic error and overtreatment of fake news “UTIs” that are not, in fact, infections.
2/
2/
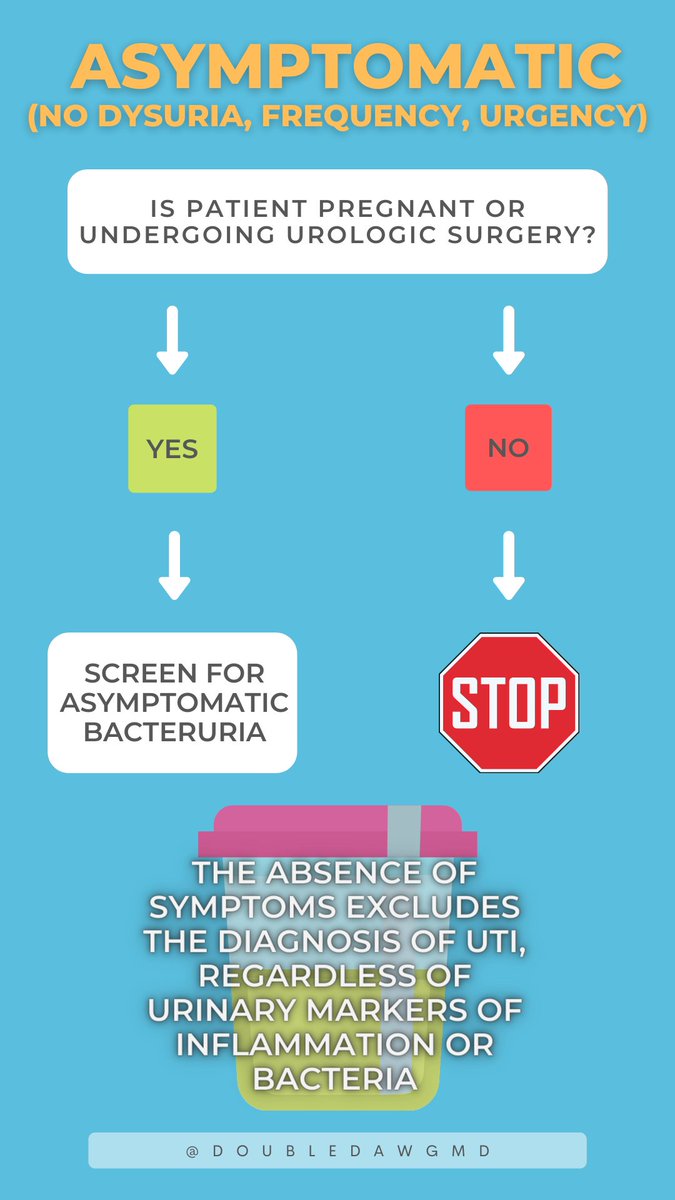
We prevent lots of harm to patients when we remember that UTI is a clinical diagnosis based on symptoms and not UA criteria.
So when ordering a UA for renal/metabolic reasons – tell yourself in advance:
INFLAMMATION = INFECTION
BACTERIA = INFECTION
3/
So when ordering a UA for renal/metabolic reasons – tell yourself in advance:
INFLAMMATION = INFECTION
BACTERIA = INFECTION
3/
The classic “infectious” portion of the UA includes both chemical (LE, nitrites) and microscopic (WBC, bacteria) components.
Take the pretest below and test your knowledge before we dive a little deeper.
4/
Take the pretest below and test your knowledge before we dive a little deeper.
4/
https://twitter.com/DoubleDawgMD/status/1409927371851960327?s=19
A + leukocyte esterase may be seen in GU inflammation, irritation from catheterization, glomerulonephritis, UTIs and STIs. It has a good negative predictive value, so is useful at ruling out disease. Because it’s not specific, it is not good at ruling in disease (low PPV).
5/
5/
Likewise, + WBCS in the urine (pyuria) has low PPV. Pyuria occurs in up to 32% of young women, 90% of elderly patients in long-term care facilities and HD patients with asymptomatic bacteriuria. The absence of pyuria is therefore much more useful than it’s presence on UA.
6/
6/
Urinary nitrites are meant to detect nitrate-reducing bacteria (classically gram negative). This is generally considered a more specific test (up to 95%), but did you know false + can occur from just exposing the urine sample to air? It can also occur with phenazopyridine.
7/
7/
The bigger issue with nitrites is that it is basically a clinically useless test. The fact that bacteria are in the urine means nothing to me unless the patient is pregnant, having urologic procedure, or symptomatic. The graphs below illustrate my point:
8/
cc: @grepmeded
8/
cc: @grepmeded

For these reasons, @Sonali_Advani and @TheQualityDoc argue that we should consider splitting the UA into its component parts and order separately based on clinical question.
Recall that more testing (esp in a population w/ low rates of dx) will lead to high false + rates.
9/
Recall that more testing (esp in a population w/ low rates of dx) will lead to high false + rates.
9/

Full paper is linked here: tinyurl.com/mrarrje It's a masterclass on the UA and a must read for all levels of learners.
@DukeIMChiefs @MayoClinicINFD @k_vaishnani @RosenelliEM @IDdocAdi @reverendofdoubt
#medtwitter #MedStudentTwitter #IDtwitter
Fin/
Was this helpful?
@DukeIMChiefs @MayoClinicINFD @k_vaishnani @RosenelliEM @IDdocAdi @reverendofdoubt
#medtwitter #MedStudentTwitter #IDtwitter
Fin/
Was this helpful?
A clarification about tweet 3:
my copy/paste of the =/= sign just ended up as =
Womp womp. The point is that inflammation and bacteria do NOT equal infection 🙃
Where's that edit button when you need it?
my copy/paste of the =/= sign just ended up as =
Womp womp. The point is that inflammation and bacteria do NOT equal infection 🙃
Where's that edit button when you need it?
Otra versión en Español 👇
Por favor, ¡Aconsejame si necesita correcciones o cambios! 🙏🏻🙏🏻🙏🏻 @MariaMjaleman @AndreaAnampaG @kiaracamacho96 @nefrorantes @medpedshosp @CarlosdelRio7
Por favor, ¡Aconsejame si necesita correcciones o cambios! 🙏🏻🙏🏻🙏🏻 @MariaMjaleman @AndreaAnampaG @kiaracamacho96 @nefrorantes @medpedshosp @CarlosdelRio7


• • •
Missing some Tweet in this thread? You can try to
force a refresh


