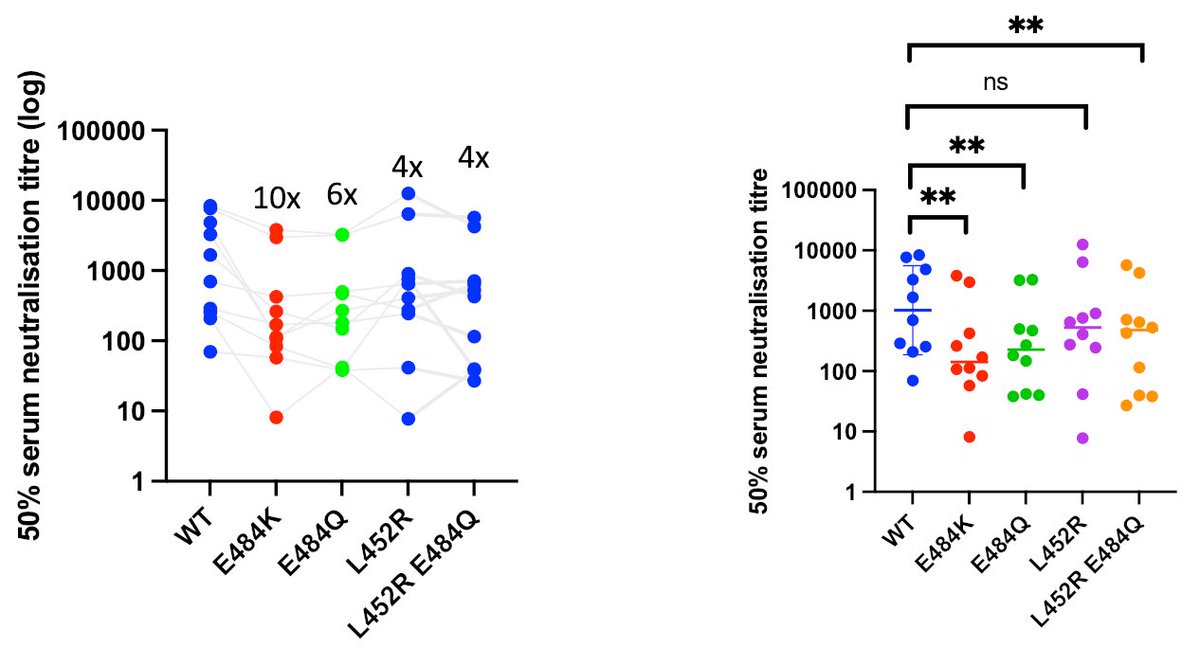
Sharing our updated pre-print on Delta Variant and emergence, replication and immune evasion properties. We previously reported partial evasion of neutralising antibody responses following vaccination and breakthrough in vaccinated health care workers. biorxiv.org/content/10.110…
We now further define Delta immune evasion using a panel of 38 monoclonal antibodies, showing significant loss of potency of NTD and RBD targeting antibodies. Imdevimab, part of the REGN2 dual monoclonal antibody cocktail is compromised by Delta. 

We also show loss of activity for casivirimab, part of the Lily dual therapy cocktail. These dual therapies could be less effective against Delta particularly in the setting of immune compromise could lead to escape variants emerging/ transmitting.
Taking replication we originally showed increased growth of Delta virus in vitro using airway organoids compared to Alpha. Now we show increased virus production in two other systems: Calu-3 epithelial lung cell lines (shown here) and airway epithelial cells (@wendybarclay11)
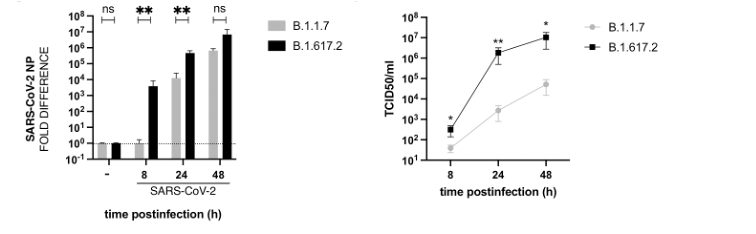
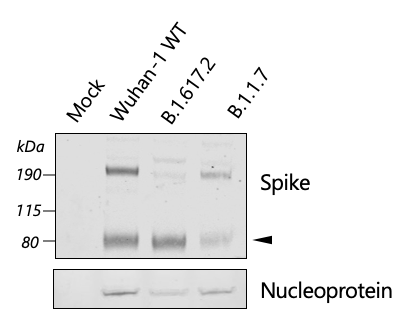
We also found that the Delta virus appears to be in a predominantly cleaved form as compared to Alpha. This may suggest that each virus particle is more infectious in addition to more virus particles being produced
These properties likely explain vaccine breakthrough. We provide data on 132 Delta infections in partially/fully vaccinated hospital staff (25% non-Delta and 75% Delta). We found ChAdOx-1 efficacy to be lower against Delta compared to non-Delta in those who received two doses.
• • •
Missing some Tweet in this thread? You can try to
force a refresh