
We know vaccines reduce your risk of infection, but they aren't *perfect.* Then what fraction of transmission in the population is from the vaccinated? How might this change with new variants?
In the thread below, I share a mental model with worked examples. 1/11
In the thread below, I share a mental model with worked examples. 1/11


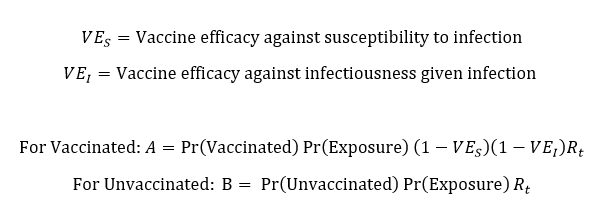
First, some definitions. We are familiar with vaccine efficacy (VE) against disease. This was estimated from trials. But many studies have helped us estimate VE against all infection (aka VE_S). For mRNA vaccines against early strains, this has hovered around 80-90%. 2/11
Even if infected, are vaccine breakthroughs less likely to transmit? Due to lower viral load, shorter illness, location of replication (nose, lungs). This is VE against infectiousness (aka VE_I). A recent preprint estimated 50% (w/ high uncertainty). 3/11
medrxiv.org/content/10.110…
medrxiv.org/content/10.110…
How often vaccinated individuals go on to transmit also depends upon:
- The level of exposure in the community
- The fraction of people vaccinated
- The reproduction number R_t
4/11
- The level of exposure in the community
- The fraction of people vaccinated
- The reproduction number R_t
4/11
But in order to approximate the relative contribution of the two groups to transmission (the fraction A/(A+B)), we can simplify this down even further. If we assume exposure is similar for unvaccinated and vaccinated individuals, then several things cancel. 5/11
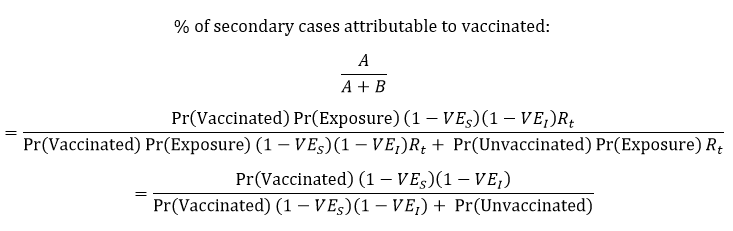
So, in this simplified model, the key is the % of the population vaccinated, plus the combination of the vaccine's effect to reduce infection and reduce infectiousness (sometimes called VE against transmission). 6/11
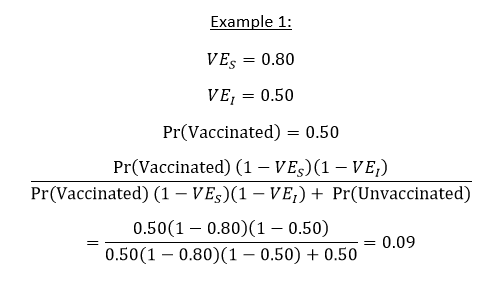
As a worked example, consider a vaccine that reduces infection by 80% and reduces infectiousness by 50%. If 50% of the population is vaccinated, about 9% of transmission is attributable to vaccinated individuals. 7/11
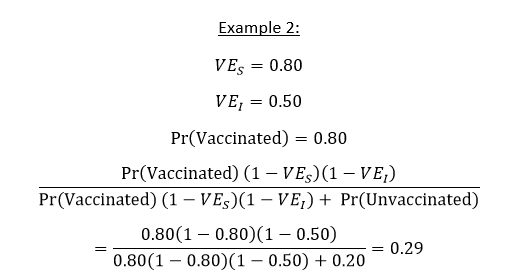
Remember this depends upon the fraction of the population vaccinated. Imagine the same vaccine but in a population with 80% vaccinated. Then the *relative* contribution of vaccinated individuals is higher, 29%, by virtue of there being more vaccinated. 8/11
[What's not captured in this simple relative contribution calculation is that, the more people who are vaccinated, the lower exposure will be for everyone! Instead I am looking just at a slice in time within a population, before the benefits accrue.] 9/11
We are still gathering evidence about the performance of these vaccines against newer variants. But we can see in this mental model how anything that erodes VE against infection or VE against infectiousness would increase the relative contribution from the vaccinated. 10/11
All the normal caveats that this is meant to be a simplified representation, but I hope it is helpful!
11/END
11/END
PS. I realize I use the word "simplified" in a few places, which I have been trying to move away from. ("It is trivial to show that..." is the worst.) I mean I made simplifying assumptions, but for those who aren't familiar with these equations, simple is the wrong word.
• • •
Missing some Tweet in this thread? You can try to
force a refresh


