
#IDDailyPearl quick Tweetorial on ART in the setting of severe renal impairment (GFR <30, not in dialysis). @erodedbyewaves and @ewelford
When CrCl <30, technically should stop TAF and FTC/3TC. TAF can be used down to CrCl 15 not on dialysis (think HBV monoinfection tx data) BUT technically FTC or 3TC should be renally-dosed at these lower CrCl.
I've seen FTC and/or 3TC continued at these lower CrCl levels since risk of lactic acidosis and/or other AE is still low but technically would not be "appropriate"
So, what then can we use?
DHHS for the win as per usual: DTG/3TC, DRV/r + 3TC, DRV/r + RAL
DHHS for the win as per usual: DTG/3TC, DRV/r + 3TC, DRV/r + RAL

Note that regimens in the last tweet were for treatment naive patients. Remember with DTG/3TC, VL must be <500,000, and no RAMs. CD4 should be >200 and VL <100,000 if using DRV/r + RAL. And all regimens don't work if chronic HBV infection present.
But who wants to use boosters? I sure don't and try to avoid it when I can!
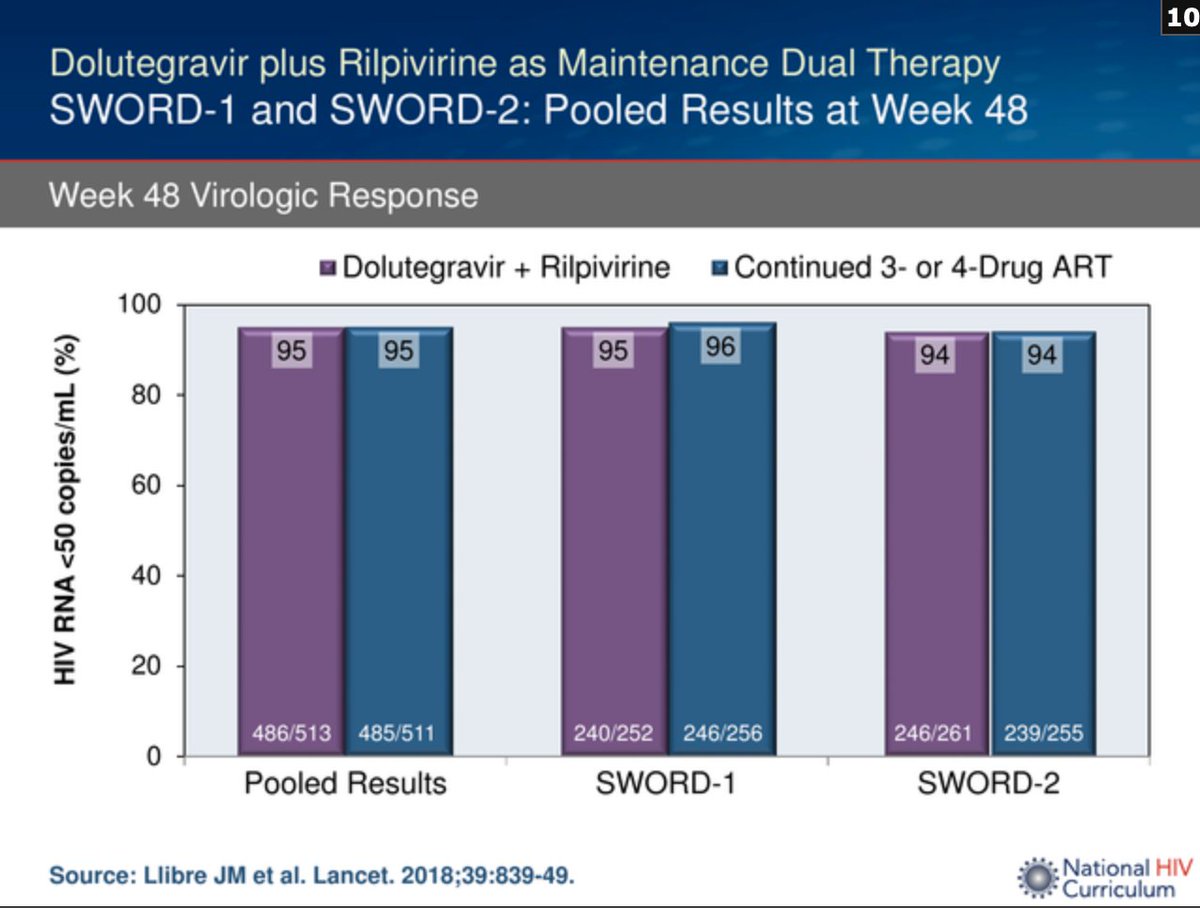
Other options: DTG/RPV (AKA Juluca). Efficacy of this regimen demonstrated in the SWORD 1 and 2 trials. Important caveats: Acid reducers with RPV are problematic, RPV requires high cal meal for optimal absorption, & cannot have HBV co-infection or RAMs.
If RPV is out due to DDIs or food requirements, another option would be Dolutegravir + Doravirine. Doravirine = newer NNRTI that doesn't have stomach acidity or large cal meal requirements. Same issues re: HBV co-infection and RAMs.
By the same logic, long-acting injectable cabotegravir + rilpivirine (Cabenuva) would be an option in renal impairment. Still have PPI/H2 blocker issue with RPV oral lead in phase and HBV co-infection and RAMs contraindications. Efficacy in ATLAS and FLAIR.

So lots of good options but need to think through, ensure no RAMs to new regimen and no chronic HBV co-infection when switching (among other details).
Sources: clinicalinfo.hiv.gov/en/guidelines/… and hiv.uw.edu/page/treatment…
Sources: clinicalinfo.hiv.gov/en/guidelines/… and hiv.uw.edu/page/treatment…
• • •
Missing some Tweet in this thread? You can try to
force a refresh













