
💥Parathyroid Hormone-related Protein - PTHrP
⚡️Who was the first person to postulate the existence of PTHrP?
⚡️What is the mechanism of PTHrP mediated hypercalcemia of malignancy?
⚡️Does PTHrP have a physiological function?
#Onconephrology
#PTHrP
1/
⚡️Who was the first person to postulate the existence of PTHrP?
⚡️What is the mechanism of PTHrP mediated hypercalcemia of malignancy?
⚡️Does PTHrP have a physiological function?
#Onconephrology
#PTHrP
1/
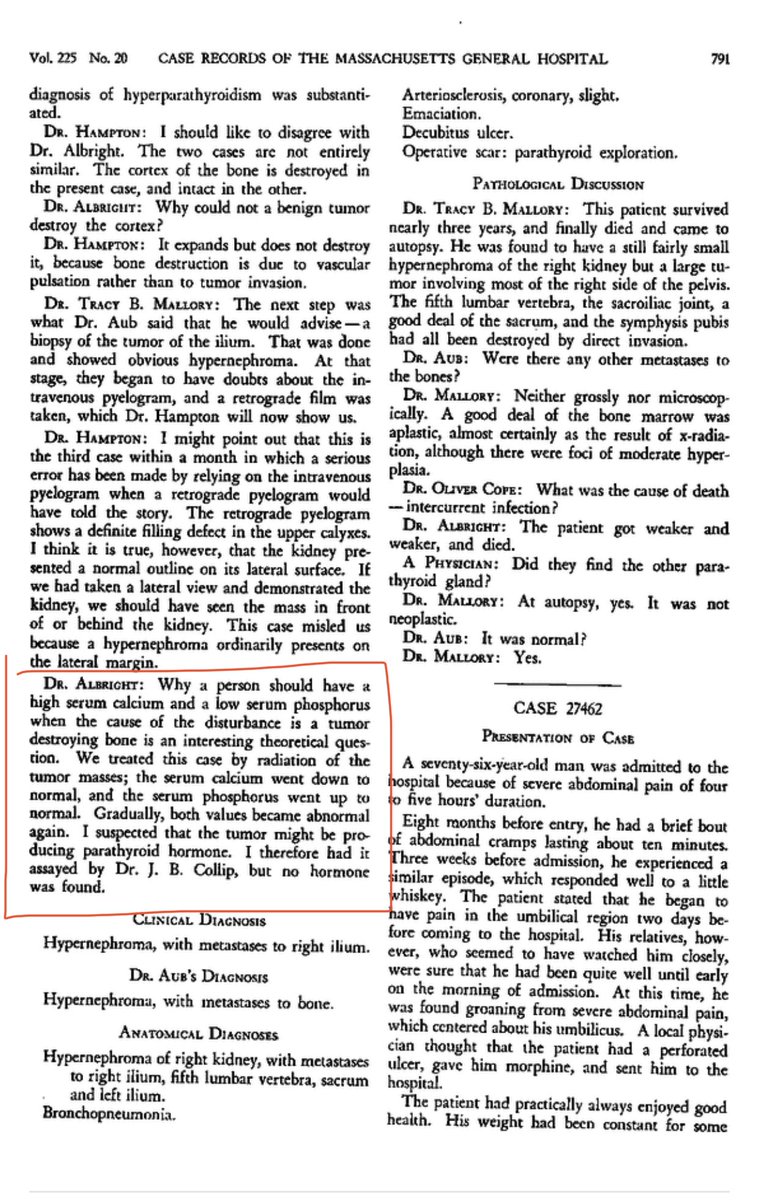
Dr. Fuller Albright, in 1941, was the first to postulate the presence of a ‘substance’ that caused features of hyperparathyroidism in a cancer patient
2/
2/
In this report, Dr. Albright essentially described the presence of PTH-like hormone in a cancer patient.
“I suspected that the tumor might be producing PTH. I therefore had it assayed but no PTH hormone was found”-Albright👇🏽
3/
nejm.org/doi/full/10.10…
“I suspected that the tumor might be producing PTH. I therefore had it assayed but no PTH hormone was found”-Albright👇🏽
3/
nejm.org/doi/full/10.10…
You may recognize Fuller Albright’s name as he is also credited for describing the McCune-Albright Syndrome.
Here is the link to Fuller Albright’s biographical sketch
pubmed.ncbi.nlm.nih.gov/21384213/
4/
Here is the link to Fuller Albright’s biographical sketch
pubmed.ncbi.nlm.nih.gov/21384213/
4/

Albright’s report was published in 1941 but it wasn’t until 1980 that ⬆️ excretion of nephrogenous cyclic AMP was described as a marker of humorally-mediated hypercalcemia of malignancy
- that humoral factor turned out to be PTHrP
pubmed.ncbi.nlm.nih.gov/6253785/
5/
- that humoral factor turned out to be PTHrP
pubmed.ncbi.nlm.nih.gov/6253785/
5/

The protein was finally purified & sequenced using cell line from squamous cell carcinoma of the lung from a pt. with hypercalcemia of malignancy.
The protein had structural & functional similarities to PTH.
It was named PTHrP👇🏽
pubmed.ncbi.nlm.nih.gov/2885845/
6/
The protein had structural & functional similarities to PTH.
It was named PTHrP👇🏽
pubmed.ncbi.nlm.nih.gov/2885845/
6/

Time for a poll question:
-PTHrP mediated hypercalcemia of malignancy is due to:
⬆️ Bone resorption, ⬆️ renal distal tubular reabsorption of calcium and ⬆️ calcium absorption from the intestine
7/
-PTHrP mediated hypercalcemia of malignancy is due to:
⬆️ Bone resorption, ⬆️ renal distal tubular reabsorption of calcium and ⬆️ calcium absorption from the intestine
7/
PTHrP has several structural & functional similarities with PTH as both
⬆️ Bone resorption
⬆️ Renal distal tubular calcium reabsorption
⬇️ Renal proximal tubular phosphate reabsorption
8/
⬆️ Bone resorption
⬆️ Renal distal tubular calcium reabsorption
⬇️ Renal proximal tubular phosphate reabsorption
8/
BUT unlike PTH, PTHrP is less likely to increase 1,25 vitamin D production so PTHrP does not increase intestinal calcium absorption
9/
9/
In 1992, this publication in Lancet showed that PTHrP accounted for hypercalcemia of malignancy in up to 80% of cancer patients👇🏽
pubmed.ncbi.nlm.nih.gov/1346019/
10/
pubmed.ncbi.nlm.nih.gov/1346019/
10/

Let’s retake the poll question:
-PTHrP mediated hypercalcemia of malignancy is due to:
⬆️ Bone resorption, ⬆️ renal distal tubular reabsorption of calcium and ⬆️ calcium absorption from the intestine
11/
-PTHrP mediated hypercalcemia of malignancy is due to:
⬆️ Bone resorption, ⬆️ renal distal tubular reabsorption of calcium and ⬆️ calcium absorption from the intestine
11/
As the role of PTHrP in hypercalcemia of malignancy became more clear, the big question was does PTHrP have a physiological function?
The answer is yes
12/
The answer is yes
12/
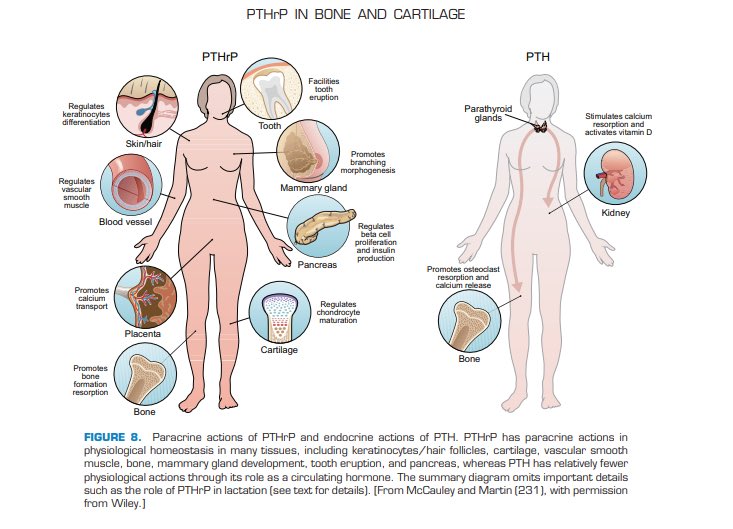
PTHrP has paracrine actions in several tissues as shown in the figure below👇🏽
PTHrP likely plays an important role in fetal development & during lactation
pubmed.ncbi.nlm.nih.gov/27142453/
13/
PTHrP likely plays an important role in fetal development & during lactation
pubmed.ncbi.nlm.nih.gov/27142453/
13/
It has been long known that fetal calcium levels are significantly higher than maternal calcium levels indicating an independent control of fetal calcium, and this effect was found to be independent of PTH👇🏽
pubmed.ncbi.nlm.nih.gov/3977382/
14/
pubmed.ncbi.nlm.nih.gov/3977382/
14/

Animal studies have shown that PTHrP stimulates placental calcium transfer to fetus which allows for mineralization of the fetal skeleton👇🏽
-In mice w/ PTHrP gene deletion fetal calcium is significantly lower than in mice w/ PTHrP
pubmed.ncbi.nlm.nih.gov/18258656/
15/
-In mice w/ PTHrP gene deletion fetal calcium is significantly lower than in mice w/ PTHrP
pubmed.ncbi.nlm.nih.gov/18258656/
15/

PTHrP is produced by the lactating mammary gland & it activates bone resorption to mobilize skeletal calcium stores
PTHrP likely plays a role in modulating calcium concentration in breast milk & lactation associated bone loss
pubmed.ncbi.nlm.nih.gov/1517711/
16/
PTHrP likely plays a role in modulating calcium concentration in breast milk & lactation associated bone loss
pubmed.ncbi.nlm.nih.gov/1517711/
16/
Summary:
⚡️Presence of PTHrP was postulated by Dr. Fuller Albright in 1941
⚡️PTHrP causes humoral hypercalcemia of malignancy
⚡️PTHrP has several paracrine functions including fetal skeletal mineralization & modulation of calcium in breast milk
End/
⚡️Presence of PTHrP was postulated by Dr. Fuller Albright in 1941
⚡️PTHrP causes humoral hypercalcemia of malignancy
⚡️PTHrP has several paracrine functions including fetal skeletal mineralization & modulation of calcium in breast milk
End/
• • •
Missing some Tweet in this thread? You can try to
force a refresh






