
@realmedicaldoc @drjaytee87 @TChivese
Loooooong thread...
1. IVM and HCQ when you look at the mechanism of action and where they act in the pathway of viral infection, it is logical and scientific to try their use. However, the key issue comes to the clinical trials.
Loooooong thread...
1. IVM and HCQ when you look at the mechanism of action and where they act in the pathway of viral infection, it is logical and scientific to try their use. However, the key issue comes to the clinical trials.
2. To make claims on efficacy of a drug, there is a standard level of evidence which has to come through carefully designed and rigorous trials so that the level of evidence is not doubted or questioned. I will put down some of the summaries from the main studies below
3. Randomized, double-blind, placebo-controlled trial in Cali, Colombia (n = 476) IVM (n = 200) and placebo (n = 198) in primary analysis. Key limitation small sample size, primary endpoint modified, sample size composition, only 4 hospitalized patients out of 398,high IVM dose 

4. Ivermectin Versus Ivermectin Plus Doxycycline Versus Placebo for Treatment of COVID-19
Randomized, double-blind, placebo-controlled trial of hospitalized adults in Dhaka, Bangladesh (n = 72)
Key limitations highlighted in the screenshot below
Randomized, double-blind, placebo-controlled trial of hospitalized adults in Dhaka, Bangladesh (n = 72)
Key limitations highlighted in the screenshot below

5. Effectiveness and Safety of Adding Ivermectin to Treatment in Patients With Severe COVID-19
Randomized, single-blind trial of hospitalized adults in Turkey (n = 66)
Randomized, single-blind trial of hospitalized adults in Turkey (n = 66)

6. Chloroquine, Hydroxychloroquine, or Ivermectin in Patients With Severe COVID-19.
Randomized, double-blind, Phase 2 trial of hospitalized adults in Brazil (n = 168)
Randomized, double-blind, Phase 2 trial of hospitalized adults in Brazil (n = 168)

7. Ivermectin Versus Placebo for Outpatients With Mild COVID-19.
Open-label RCT of adult outpatients in Lahore, Pakistan (n = 50)
Open-label RCT of adult outpatients in Lahore, Pakistan (n = 50)

8. Ivermectin in Patients With Mild to Moderate COVID-19. Open-label, single-center, RCT of outpatients with laboratory-confirmed SARS-CoV-2 infection in Bangladesh (n = 62)

9. Ivermectin Plus Doxycycline Versus Hydroxychloroquine Plus Azithromycin for Asymptomatic Patients and Patients With Mild to Moderate COVID-19.
RCT of outpatients with SARS-CoV-2 infection with or without symptoms in Bangladesh (n = 116)
This is a preliminary report no peer rev
RCT of outpatients with SARS-CoV-2 infection with or without symptoms in Bangladesh (n = 116)
This is a preliminary report no peer rev

10. Antiviral Effect of High-Dose Ivermectin in Adults with COVID-19. Multicenter, randomized, open-label, blinded trial of hospitalized adults with mild to moderate COVID-19 in Argentina (n = 45).

11. Effect of Early Treatment With Ivermectin Versus Placebo on Viral Load, Symptoms, and Humoral Response in Patients With Mild COVID-19. A single-center, randomized, double-blind, placebo-controlled pilot trial in Spain (n = 24)

12. Ivermectin Plus Doxycycline Plus Standard Therapy Versus Standard Therapy Alone in Patients With Mild to Moderate COVID-19. Randomized, unblinded, single-center study of patients with laboratory-confirmed SARS-CoV-2 infection in Baghdad, Iran (n = 140) *not published yet.

13. Ivermectin in Patients With Mild to Moderate COVID-19. Double-blind RCT in patients with mild to moderate COVID-19 in India (n = 157)

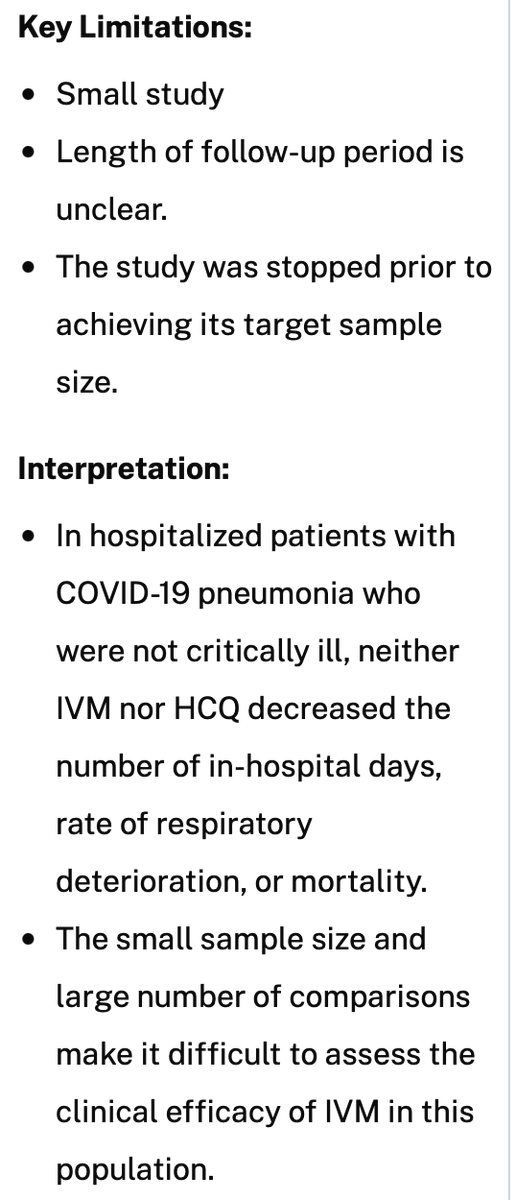
14. Efficacy and Safety of Ivermectin and Hydroxychloroquine in Patients With Severe COVID-19.
Randomized, double-blind trial of hospitalized adults with COVID-19 pneumonia in Mexico (n = 106) *not yet peer reviewed.
Randomized, double-blind trial of hospitalized adults with COVID-19 pneumonia in Mexico (n = 106) *not yet peer reviewed.
15. Ivermectin as Adjunctive Therapy to Hospitalized Patients With COVID-19. Randomized, double-blind, placebo-controlled, multicenter, Phase 2 clinical trial of hospitalized adults with mild to severe SARS-CoV-2 infection in 5 facilities in Iran (n = 180) *not yet peer reviewed.

16. Retrospective Analysis of Ivermectin in Hospitalized Patients With COVID-19. Retrospective analysis of consecutive patients with laboratory-confirmed SARS-CoV-2 infection who were admitted to 4 Florida hospitals (n = 276)

17. Observational Study on the Effectiveness of Hydroxychloroquine, Azithromycin, and Ivermectin Among Hospitalized Patients With COVID-19. Retrospective cohort study of hospitalized adults with COVID-19 in Peru (n = 5,683)..published and later RETRACTED!

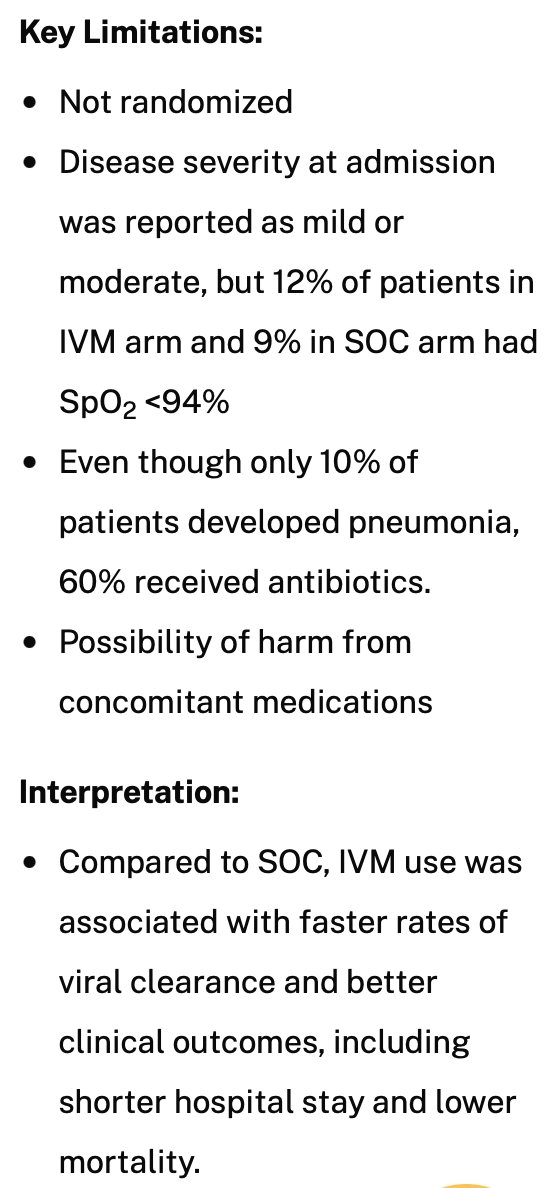
18. Retrospective Study of Ivermectin Versus Standard of Care in Patients With COVID-19. Retrospective study of consecutive adult patients hospitalized in Bangladesh with laboratory-confirmed SARS-CoV-2 infection (n = 248). *prelim report not peer reviewed...will check update
19. The full assessment of these studies is available here:
covid19treatmentguidelines.nih.gov/tables/table-2…
This website was last updated on July 19, 2021.
covid19treatmentguidelines.nih.gov/tables/table-2…
This website was last updated on July 19, 2021.
20. So there is a lot that has happened over the last year pertaining the use of IVM. There was a lot of noise made over the SA authorities using or not using it and the controversy continues. The best way to resolve this is to have a large study n > 10000 (just wild guess)
21. The clear trend is that the sample size and study design issues are the principal source of reservation in terms of its use. My position is, if it works then use it, but let us do the necessary studies in our own scenario and publish.
22. Let those who want it lobby for the clinical trials to be done so that we can quickly make a decisive position on including it as part of the cocktail against COVID-19. We can debate till tomorrow but let the data be clear. Govt can coordinate these trials easily, do it.
23. Let us hear what other people think....✌🏾✌️
@threadreaderapp unroll
• • •
Missing some Tweet in this thread? You can try to
force a refresh


