
If anyone needs a good 😂 this is the figure from the China-WHO report showing the home address of covid-19 cases from Dec 11, 2019 or earlier.
A team of scientists, unable to access early case data, had no choice but to extract information from this fig using Adobe Illustrator.
A team of scientists, unable to access early case data, had no choice but to extract information from this fig using Adobe Illustrator.

Problematically, despite being already of such low resolution, the map still has 'unintended errors' as revealed by @washingtonpost
washingtonpost.com/world/asia_pac…
washingtonpost.com/world/asia_pac…
These errors are shown here in a diagram made by @InWuchang

I think it's important for @WHO to either put a huge warning label on their #OriginsOfCovid Report and Annex, or to take these down until corrections are made - before more scientists are misled by these unintended errors.
who.int/docs/default-s…
who.int/docs/default-s…
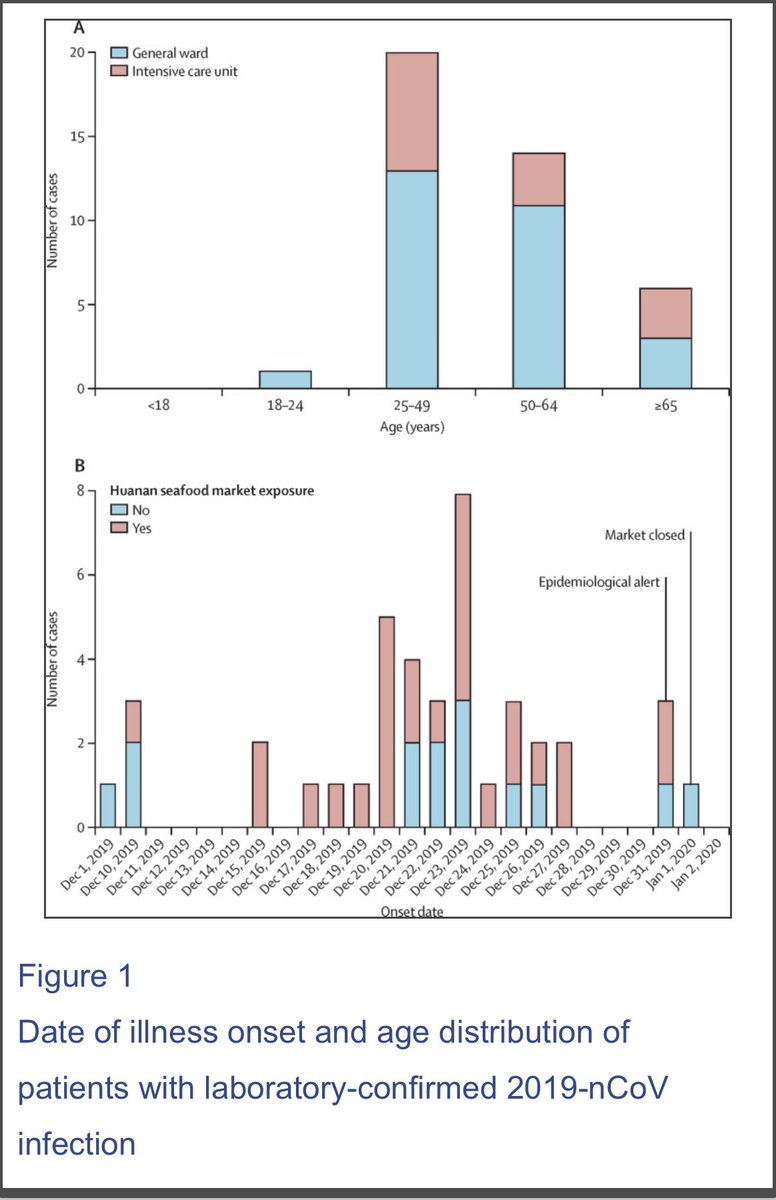
At the bare minimum, the authors of this Lancet study should be consulted to match their 41 lab-confirmed covid cases (Dec 2019-Jan 2, 2020) to this map - can it be done?
ncbi.nlm.nih.gov/pmc/articles/P…
ncbi.nlm.nih.gov/pmc/articles/P…
Who is this person and which district did they live in? “The symptom onset date of the first patient identified was Dec 1, 2019. None of his family members developed fever or any respiratory symptoms. No epidemiological link was found between the first patient and later cases.”
We can see from the Lancet study that these 41 cases were most likely the tip of the iceberg even in Dec 2019. Large portion of the patients were in ICU even if young, not many cases below 25 years of age.
Earliest cases no link to the Huanan seafood market.
Earliest cases no link to the Huanan seafood market.
I think it’s useful to consult other maps of covid-19 cases even if these cover more Jan 2020 cases… why do these show greater case density in the district where the Huanan market wasn’t located but the WIV campus was?
https://twitter.com/inwuchang/status/1424347301695348741
That being said, I think over-reliance on a map of early cases by home address (especially one that cannot be independently reproduced due to lack of access to data) can mislead the search for the origin of Covid-19. ayjchan.medium.com/a-response-to-…
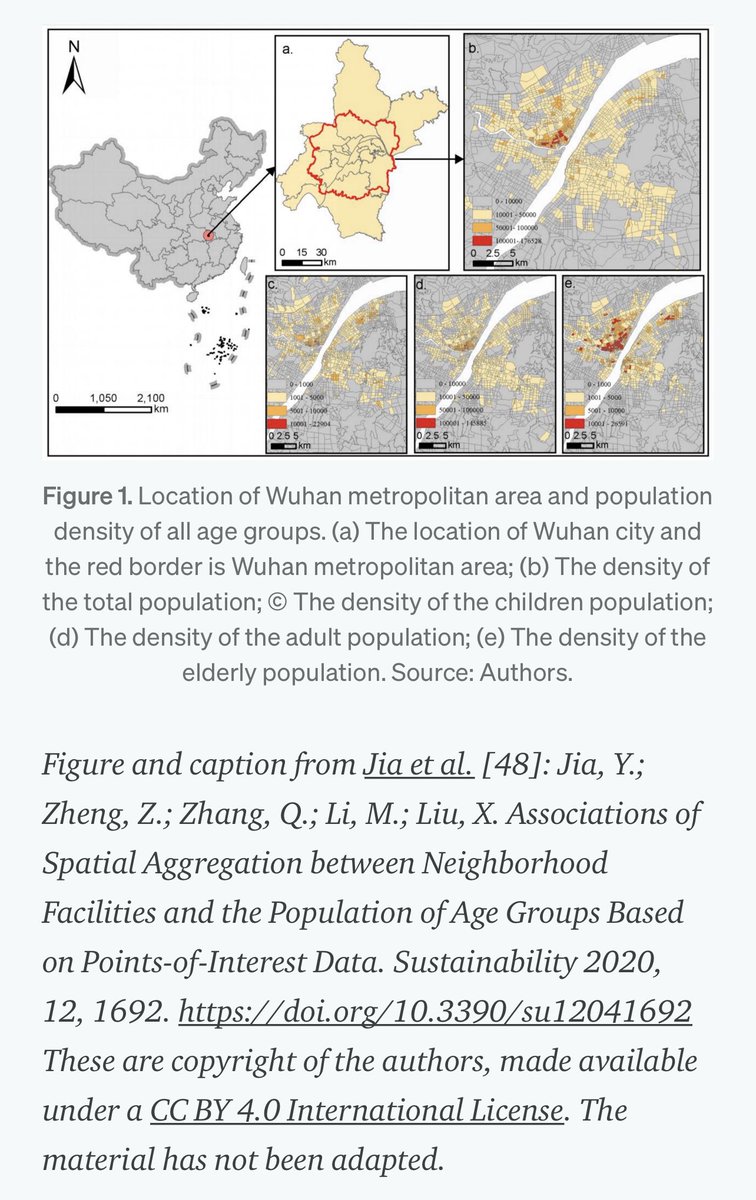
The early covid-19 case map from WHO (left) looks strikingly similar to the distribution of general population & elderly in Wuhan (right).
My bet is they were only seeing the worst Dec 2019 cases - making sense these map to most crowded parts of the city with the most elderly.
My bet is they were only seeing the worst Dec 2019 cases - making sense these map to most crowded parts of the city with the most elderly.

We also know from the China-WHO report that the criteria by which early cases had been identified suffered from ascertainment biases (Annex E3).
Exposure to the Huanan market was one of the key factors in determining whether a patient was a suspected case of Covid-19.
Exposure to the Huanan market was one of the key factors in determining whether a patient was a suspected case of Covid-19.
To be a suspected case you had to have at least two clinical manifestations, i.e., fever, (pulmonary) imaging characteristic of pneumonia, reduction in WBC/lymphocyte, or no improvement in response to three days of antibiotics.
I’d say this skews towards elderly cases.
I’d say this skews towards elderly cases.
Previous examples of natural spillovers and lab-acquired infections illustrate the importance of tracking down the earliest patients and identifying their exposures to various possible sources of the pathogen.
In a city, home address almost has no bearing on tracking origin.
In a city, home address almost has no bearing on tracking origin.
For example, a Beijing researcher who was accidentally infected with SARS-CoV in 2004 was not actually the first case in the cluster to be diagnosed; a nurse that had treated the researcher was the first diagnosed…
Would the nurse’s home address be useful?
Would the nurse’s home address be useful?
Furthermore, the researcher had traveled long distances via train across China while symptomatic. Another three researchers at the same institute were later found to have been separately infected with SARS-CoV.
Would all of their home addresses in Beijing be useful?
Would all of their home addresses in Beijing be useful?
What matters is interviewing the early cases, getting their occupations and history of activities/exposures running up to when symptoms appeared. If the patients are not available, the doctors who tracked their cases (and blew the whistle) should be consulted.
Has this happened?
Has this happened?
• • •
Missing some Tweet in this thread? You can try to
force a refresh




