
1/
The overall effects of this study are miniscule—0.07% absolute reduction in seroprevalence. But the topline finding is “We decreased seroprevalence by 10%!”
Technically true...
But even this finding is questionable. Let's explore.
poverty-action.org/sites/default/…
The overall effects of this study are miniscule—0.07% absolute reduction in seroprevalence. But the topline finding is “We decreased seroprevalence by 10%!”
Technically true...
But even this finding is questionable. Let's explore.
poverty-action.org/sites/default/…

2/2/
What the study ACTUALLY measures is the impact of mask promotion on symptom reporting. Only if a person reports symptoms, are they asked to participate in a serology study—and only 40% of those with symptoms chose to have their blood taken.
What the study ACTUALLY measures is the impact of mask promotion on symptom reporting. Only if a person reports symptoms, are they asked to participate in a serology study—and only 40% of those with symptoms chose to have their blood taken.

3/ Is it possible that that highly moralistic framing and monetary incentives given to village elders for compliance might dissuade a person from reporting symptoms representing individual and collective moral failure—one that could cost the village money? Maybe?

4/
Given that the difference is tiny, if this had even a small impact, it could completely skew the results. Might the same factors be at play when an individual weighed whether or not to be tested? After all, a positive test would indicate that your village was “failing”
Given that the difference is tiny, if this had even a small impact, it could completely skew the results. Might the same factors be at play when an individual weighed whether or not to be tested? After all, a positive test would indicate that your village was “failing”

5/
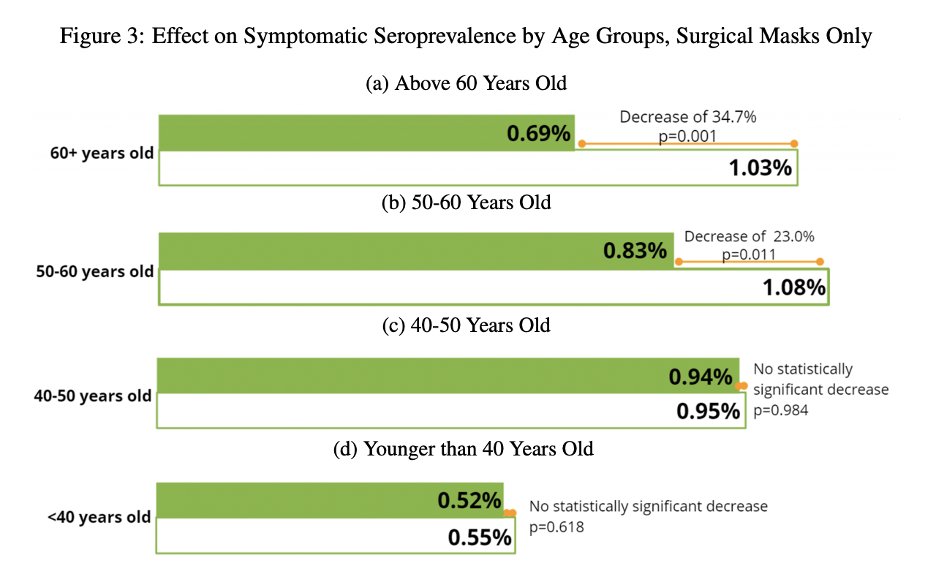
The fact that age stratification shows that interventions had no impact on younger people, but did on older people calls this finding into question. There is no physical mechanism by which universal masking would protect the elderly, but not the young.
The fact that age stratification shows that interventions had no impact on younger people, but did on older people calls this finding into question. There is no physical mechanism by which universal masking would protect the elderly, but not the young.

6/
Such a result could be explained by the mask promotion campaign creating a sense of fear that resulted in elderly sequestering themselves. If that were the case, a more elderly-targeted approach could achieve the same results.
Such a result could be explained by the mask promotion campaign creating a sense of fear that resulted in elderly sequestering themselves. If that were the case, a more elderly-targeted approach could achieve the same results.
7/
It is also possible that elderly people in intervention groups were less likely to report symptoms. 60+ are 2-3x more likely to be symptomatic than <40. Again, when having symptoms means you failed your village, might you choose not to mention them?
jamanetwork.com/journals/jaman…
It is also possible that elderly people in intervention groups were less likely to report symptoms. 60+ are 2-3x more likely to be symptomatic than <40. Again, when having symptoms means you failed your village, might you choose not to mention them?
jamanetwork.com/journals/jaman…
8/
Perhaps the most compelling aspect of the study is the difference between surgical and cloth mask villages. The authors claim that this is supported by the different filtration efficiencies of cloth and surgical masks.
Perhaps the most compelling aspect of the study is the difference between surgical and cloth mask villages. The authors claim that this is supported by the different filtration efficiencies of cloth and surgical masks.

8/
However, these filtration efficiencies are taken in a no-gap scenario. And there is ALWAYS a gap. We can see that when considering gaps—the most important element of filtration--fabric & surgical masks perform nearly identically--not at all.
However, these filtration efficiencies are taken in a no-gap scenario. And there is ALWAYS a gap. We can see that when considering gaps—the most important element of filtration--fabric & surgical masks perform nearly identically--not at all.
https://twitter.com/Emily_Burns_V/status/1398024406312620034
10/
Given physical improbability, it is possible that this effect too, might be an artifact of bias in the control group. Surgical masks are “fancier," & might feel like more of an intervention, and may make those in such a village even more likely to repress symptom reporting.
Given physical improbability, it is possible that this effect too, might be an artifact of bias in the control group. Surgical masks are “fancier," & might feel like more of an intervention, and may make those in such a village even more likely to repress symptom reporting.

11/
Whatever the result of the surgical masks, this shows that the impact from cloth masks is 0. (.02% absolute reduction and a p-value of 0.540 is zero, even if the authors want to pretend otherwise).
Whatever the result of the surgical masks, this shows that the impact from cloth masks is 0. (.02% absolute reduction and a p-value of 0.540 is zero, even if the authors want to pretend otherwise).

12/
Color me skeptical on this one. This study increased mask wearing to 40%. In much of blue America mask compliance approached 100% for almost a year. Even with that kind of incredible compliance, there was no impact on case transmission rates.
Color me skeptical on this one. This study increased mask wearing to 40%. In much of blue America mask compliance approached 100% for almost a year. Even with that kind of incredible compliance, there was no impact on case transmission rates.
https://twitter.com/andrewbostom/status/1397248218015096838
13/
For more on why I think that these results are highly questionable, read this thread.
For more on why I think that these results are highly questionable, read this thread.
https://twitter.com/Emily_Burns_V/status/1398024406312620034
14/
Further good analysis--that gets to the heart of the matter more quickly.
Further good analysis--that gets to the heart of the matter more quickly.
https://twitter.com/federicolois/status/1433123776208777227
15/
Also good analysis.
Also good analysis.
https://twitter.com/contrarian4data/status/1433117748041633795
15/
Never underestimate the value of feline friends.
This is just brutal.
Read.it.all
boriquagato.substack.com/p/more-on-the-…
Never underestimate the value of feline friends.
This is just brutal.
Read.it.all
boriquagato.substack.com/p/more-on-the-…
• • •
Missing some Tweet in this thread? You can try to
force a refresh













