The community masking trial in Bangladesh by @Jabaluck @mushfiq_econ et al is AMAZING & EXCEPTIONALLY well done
Joy to read & I learned a LOT
Encourage all scientists in related disciplines to read, even if not your content
Thread on study
poverty-action.org/publication/im…
Joy to read & I learned a LOT
Encourage all scientists in related disciplines to read, even if not your content
Thread on study
poverty-action.org/publication/im…
2| DISCLAIMERS FIRST
1. I apply this same scientific lens to all health care & pharma trials I find interesting
2. Most relevant & needed to LMIC. But I will also take a US lens on how this may apply
I understand this is a hot button, or should we say, a hot mask issue
1. I apply this same scientific lens to all health care & pharma trials I find interesting
2. Most relevant & needed to LMIC. But I will also take a US lens on how this may apply
I understand this is a hot button, or should we say, a hot mask issue
3| TOPLINE FINDINGS
Masking worked modestly, driven nearly exclusively by surgical masks, benefits accrued to older adults, & sadly no improvement in mask wearing by any community & household strategies without sustainability in mask wearing
Masking worked modestly, driven nearly exclusively by surgical masks, benefits accrued to older adults, & sadly no improvement in mask wearing by any community & household strategies without sustainability in mask wearing
4| STUDY OVERVIEW
8-week Cluster RCT of a multi-component strategy to increase community masking, with several cross randomized strategies to answer many other important questions
primary outcome: symptomatic & seroprevalent (antibody+) COVID19
8-week Cluster RCT of a multi-component strategy to increase community masking, with several cross randomized strategies to answer many other important questions
primary outcome: symptomatic & seroprevalent (antibody+) COVID19
5| CONTEXT OF STUDY SETTING:
Bangladeshi govt mandated masks & threatened penalties for non-adherence, but only 20% wore
Bangladeshis don't think much of their govt leaders' mandates (dissimilar to US?)
Bangladeshi govt mandated masks & threatened penalties for non-adherence, but only 20% wore
Bangladeshis don't think much of their govt leaders' mandates (dissimilar to US?)

6| MORE CONTEXT
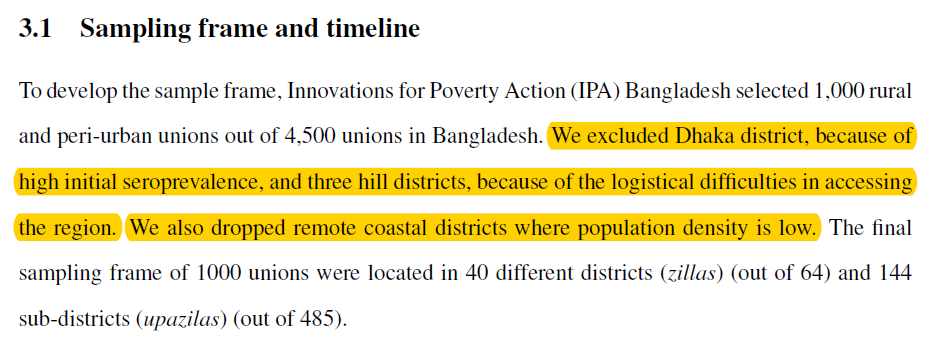
Trial didn't include Dhaka & districts where seroprevalence was high (~68%) due to mostly prior infection since vax largely unavailable
And excluded low density villages
Implied reason: too hard to show effect of mask since outcome rate would be too low!
Trial didn't include Dhaka & districts where seroprevalence was high (~68%) due to mostly prior infection since vax largely unavailable
And excluded low density villages
Implied reason: too hard to show effect of mask since outcome rate would be too low!
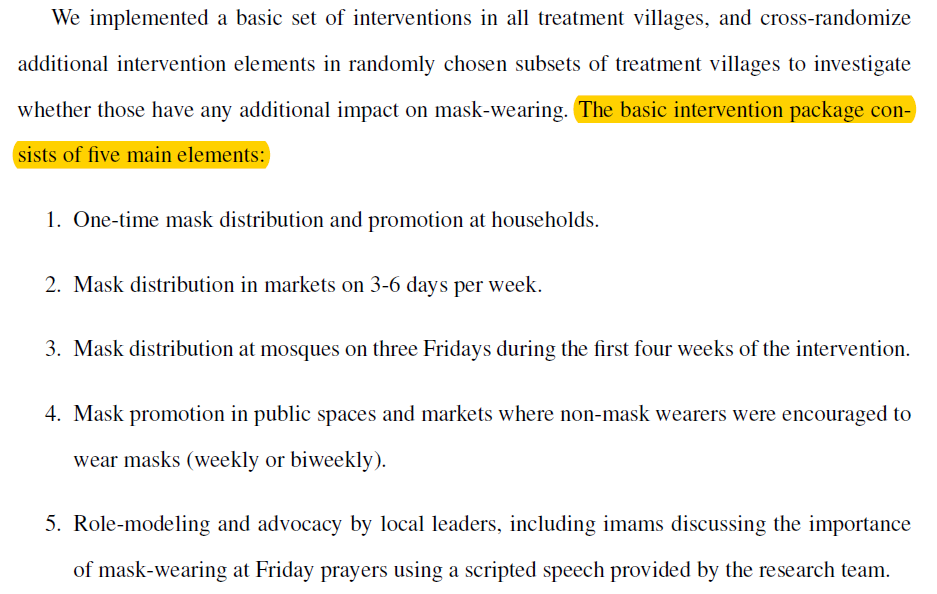
7| INTERVENTION:
multi-component strategy of free mask distribution, role modeling, and active mask promotion (the latter of which seemed critical in pilot work)
multi-component strategy of free mask distribution, role modeling, and active mask promotion (the latter of which seemed critical in pilot work)
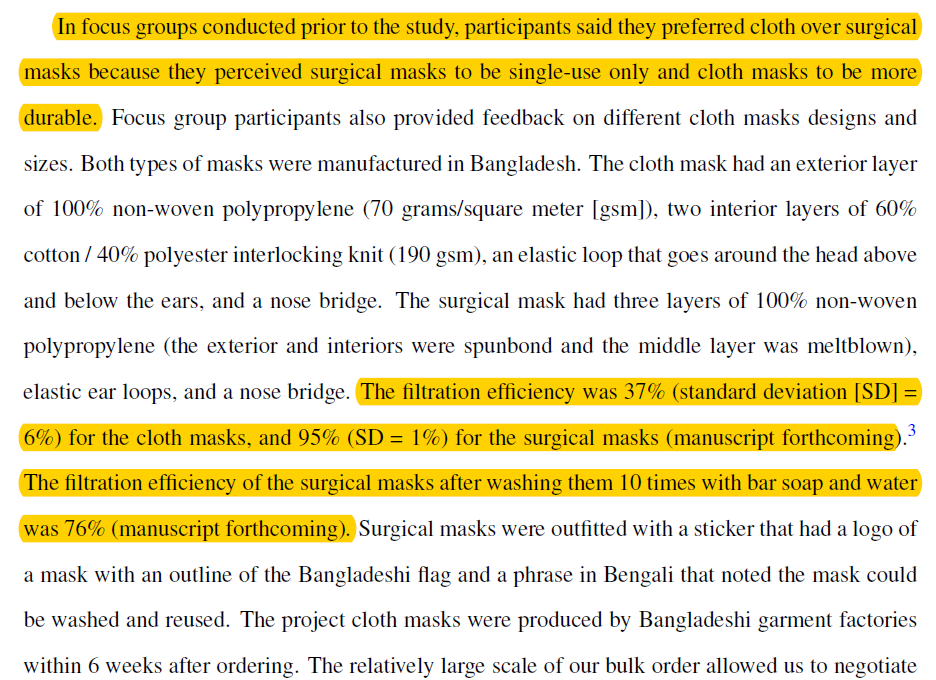
8| INTERVENTION details on cloth masks
-Beforehand participants preferred cloth masks (also what I see used most in SF)
-Cloth masks were designed for this trial & seemed better than your average bear for fit/filtration, but defer to experts if can achieve better filtration
-Beforehand participants preferred cloth masks (also what I see used most in SF)
-Cloth masks were designed for this trial & seemed better than your average bear for fit/filtration, but defer to experts if can achieve better filtration
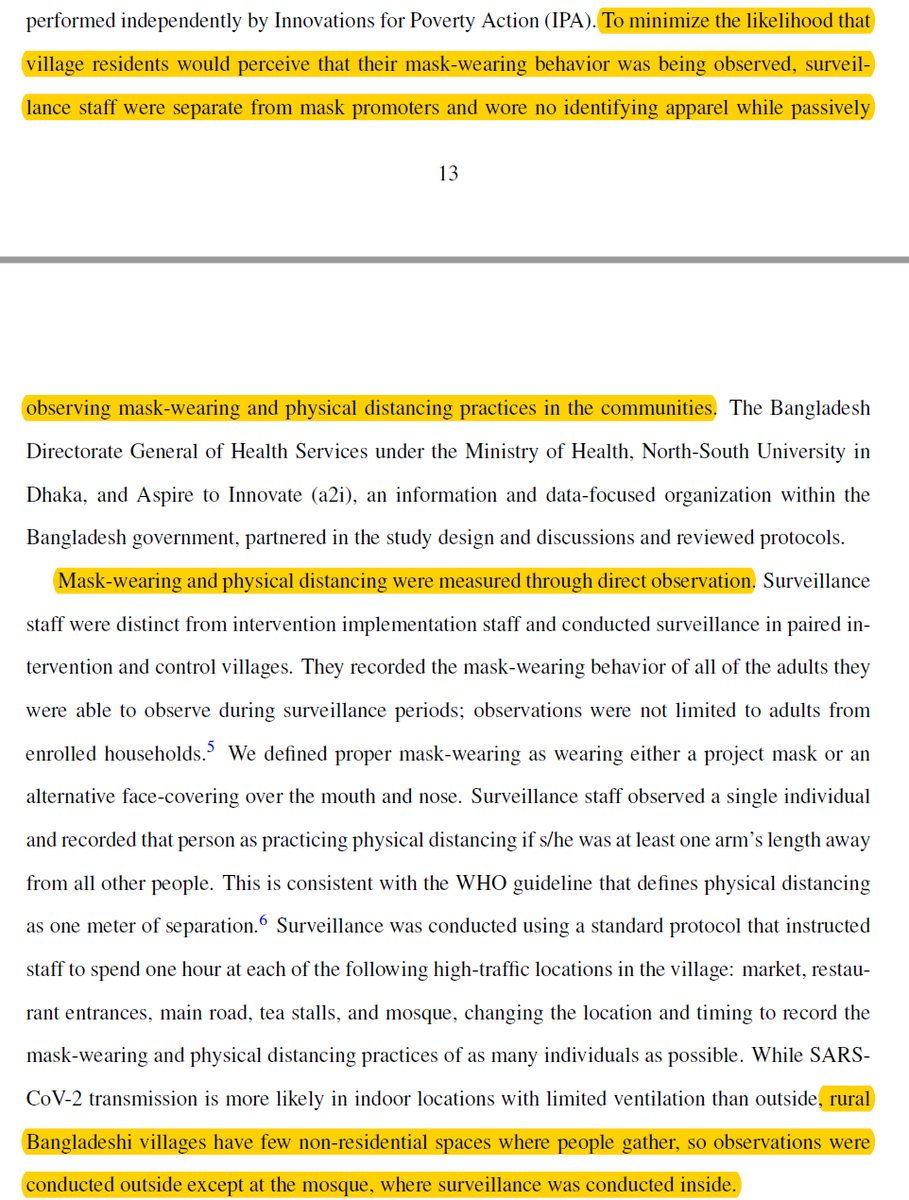
9| INTERVENTION ADHERENCE
One of my FAVORITE parts of this trial
Impressive to randomize to intervention strategy, but even more impressive to directly observe mask adherence & major co-intervention of distancing in a way to minimize Hawthorne effect bias
One of my FAVORITE parts of this trial
Impressive to randomize to intervention strategy, but even more impressive to directly observe mask adherence & major co-intervention of distancing in a way to minimize Hawthorne effect bias
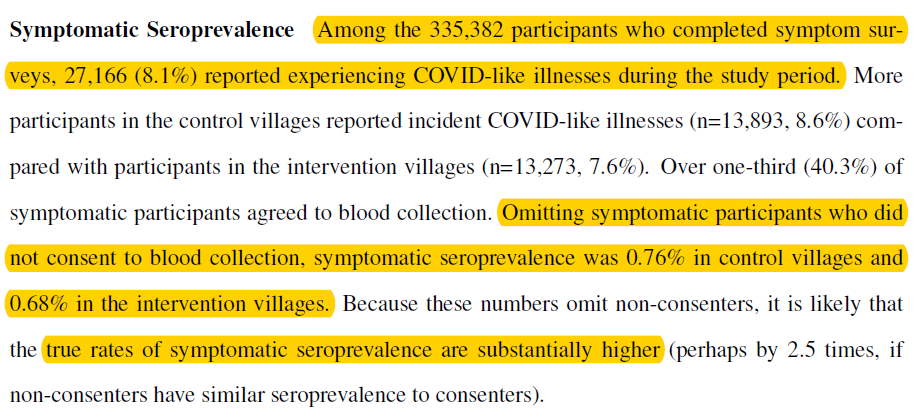
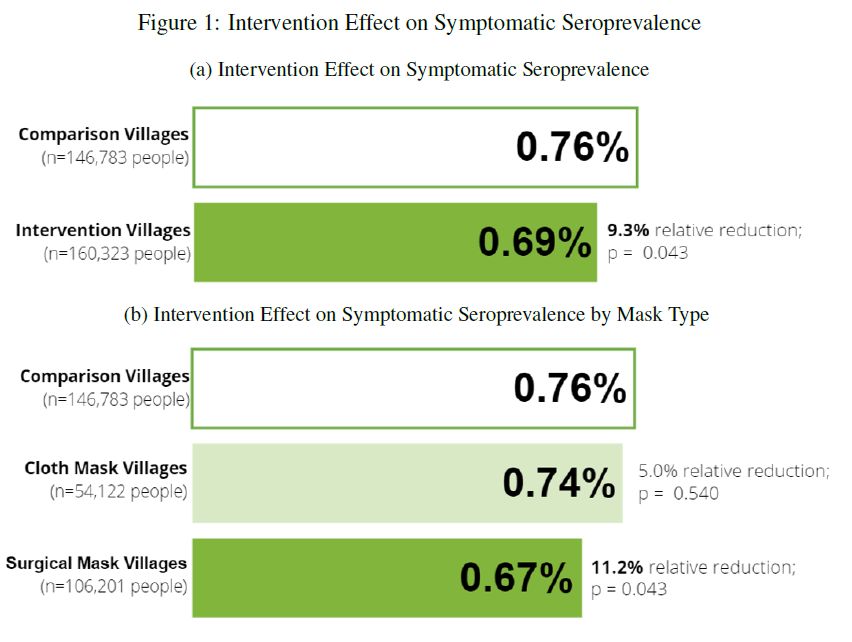
10| PRIMARY OUTCOME is symptomatic antibody+ COVID
Another favorite of mine is this more bias-resistant end point
Symptoms alone is very prone to reporting bias if you knew you wore masks & inflates outcomes ~10 fold based on findings here
Another favorite of mine is this more bias-resistant end point
Symptoms alone is very prone to reporting bias if you knew you wore masks & inflates outcomes ~10 fold based on findings here
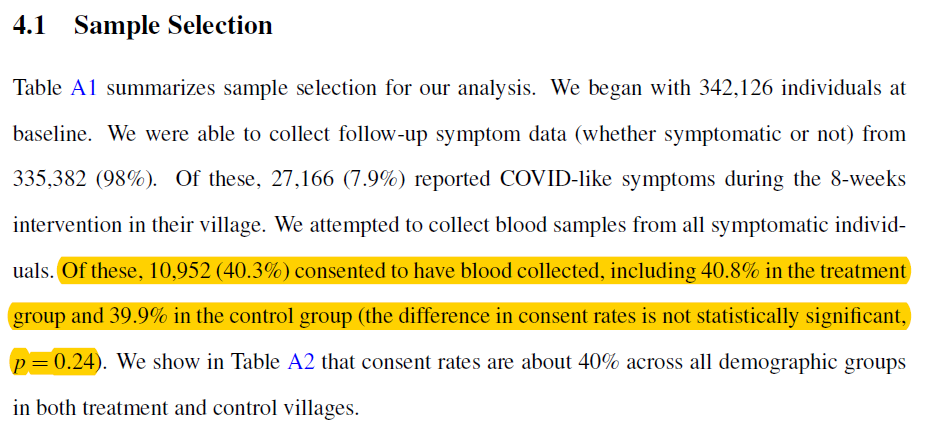
11| PRIMARY OUTCOME RATE
although only 40% of symptomatic individuals consented to blood testing for antibodies
fortunately non-differential between arms
although does decrease absolute outcome rate, by as much as 2.5 fold if similar +Ab rate in untested symptomatic people
although only 40% of symptomatic individuals consented to blood testing for antibodies
fortunately non-differential between arms
although does decrease absolute outcome rate, by as much as 2.5 fold if similar +Ab rate in untested symptomatic people
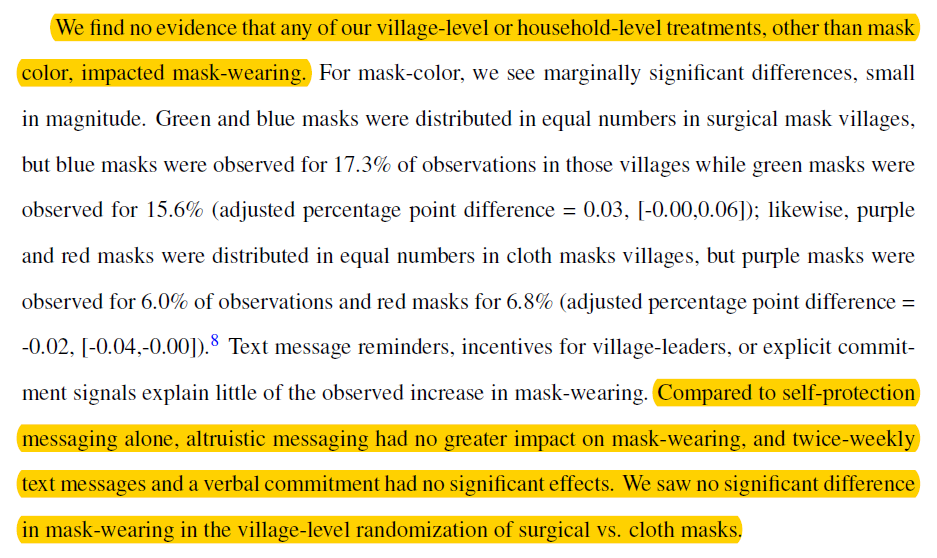
12| RESULTS ON MASK WEARING
Dramatic 29% increase in mask wearing, with largest increase in Mosques (37%)--highest risk public setting
But NO randomized community or household level intervention, except maybe mask color, increased mask wearing. Design matters. Rest not so much
Dramatic 29% increase in mask wearing, with largest increase in Mosques (37%)--highest risk public setting
But NO randomized community or household level intervention, except maybe mask color, increased mask wearing. Design matters. Rest not so much
13| RESULTS ON PHYSICAL DISTANCING
Mask intervention also led to 5% absolute increase in physical distancing in public places (markets) but not in Mosques (shoulder to shoulder among men)
This is a MAJOR co-intervention that could attenuate efficacy of masks (more later)
Mask intervention also led to 5% absolute increase in physical distancing in public places (markets) but not in Mosques (shoulder to shoulder among men)
This is a MAJOR co-intervention that could attenuate efficacy of masks (more later)
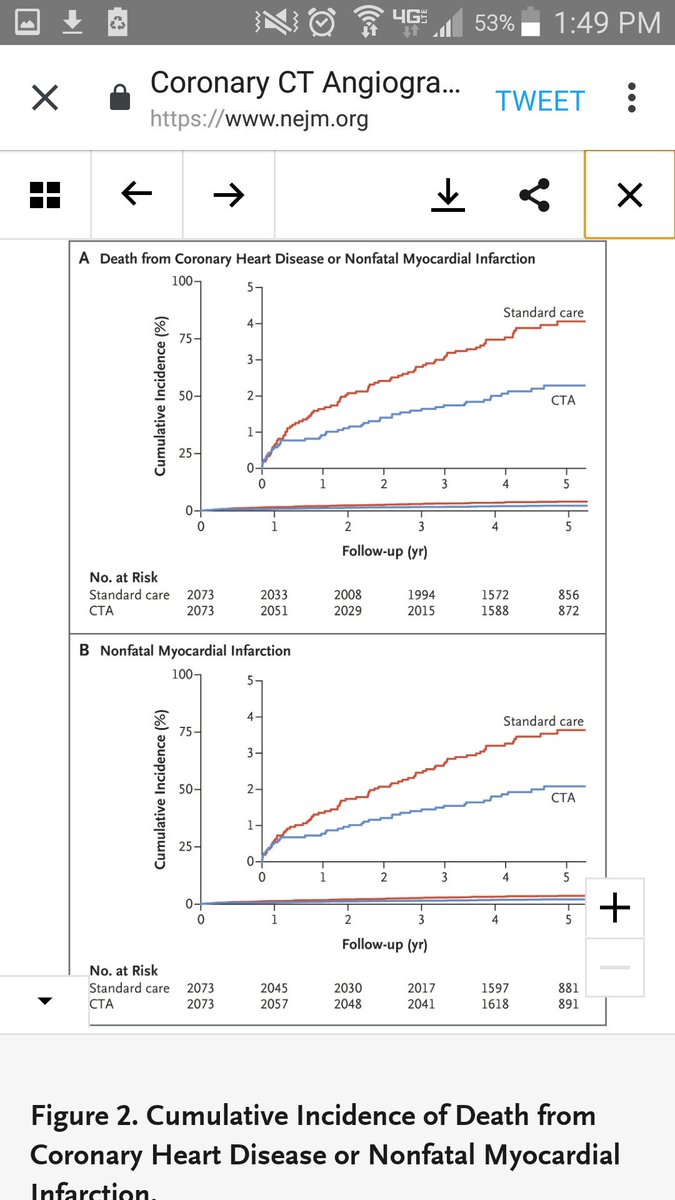
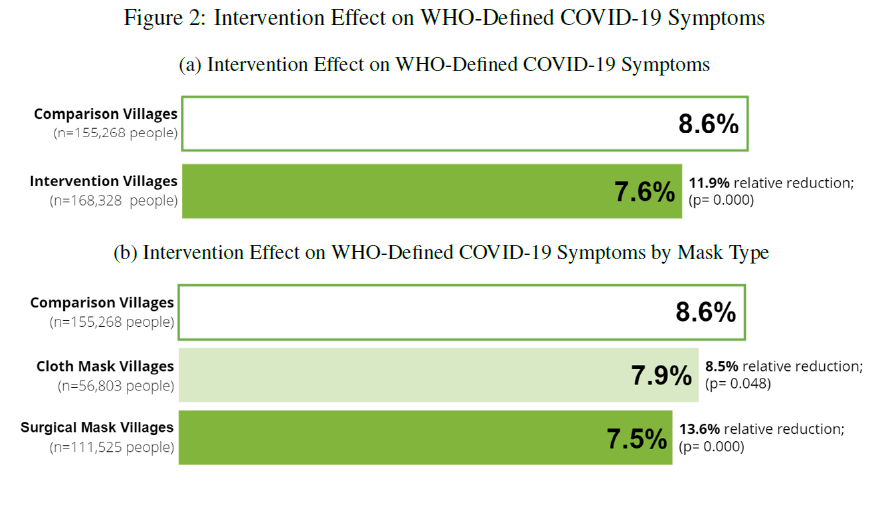
14| TOPLINE RESULTS
shown in figure on left and the much more bias-susceptible & inflated COVID outcomes on right (though could be spillover benefit from other URIs)
if wear a mask, wear a surgical mask (or better)
shown in figure on left and the much more bias-susceptible & inflated COVID outcomes on right (though could be spillover benefit from other URIs)
if wear a mask, wear a surgical mask (or better)
15| HOW DO FINDINGS APPLY TO U.S.
In high vax regions in US (like SF, vermont), absolute effect sizes would be much much smaller
also, relative effect sizes also could be smaller if vaxxed transmit less if do get COVID
In high vax regions in US (like SF, vermont), absolute effect sizes would be much much smaller
also, relative effect sizes also could be smaller if vaxxed transmit less if do get COVID
https://twitter.com/Jabaluck/status/1433082242960658432?s=20
16| WHO BENEFITTED?
Benefits accrued only to older adults in subgroup analysis
So it seems mask wearing for adults <50 is for altruism of decreasing spread to more vulnerable, but not self protection
Still IMO enough to justify widespread surgical masking with caveats
Benefits accrued only to older adults in subgroup analysis
So it seems mask wearing for adults <50 is for altruism of decreasing spread to more vulnerable, but not self protection
Still IMO enough to justify widespread surgical masking with caveats

17| DOES INTERVENTION LEAD TO PERSISTENT MASK WEARING?
Unfortunately NO
By 20 weeks (or 3 months after intervention ended), ~20% in intervention arm wore masks, which was similar to pre-intervention levels
So did not lead to sustained changes of people's hearts & minds
Unfortunately NO
By 20 weeks (or 3 months after intervention ended), ~20% in intervention arm wore masks, which was similar to pre-intervention levels
So did not lead to sustained changes of people's hearts & minds

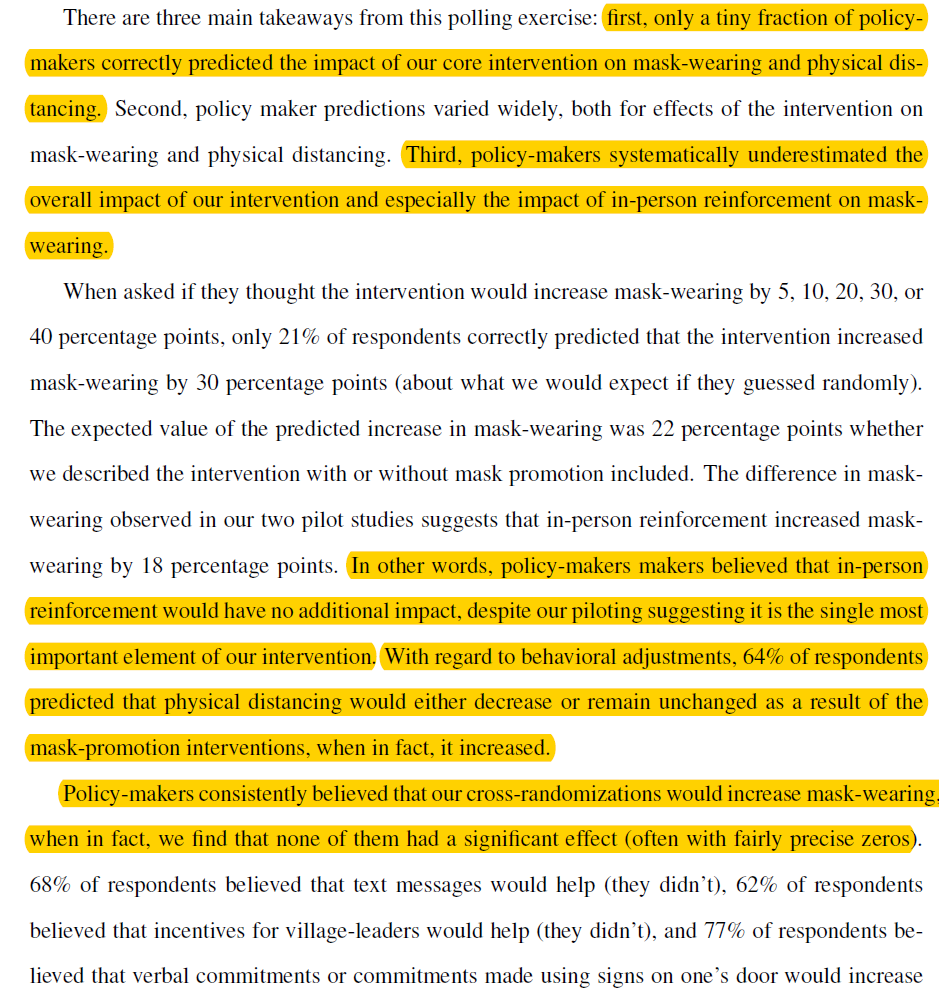
18| SO DID WE LEARN ANYTHING NEW?
In contrast to mask nihilists or cultists, we learned a lot
Much of these findings were unexpected among policy experts
This was another of my favorite parts of the trial
In contrast to mask nihilists or cultists, we learned a lot
Much of these findings were unexpected among policy experts
This was another of my favorite parts of the trial
19| MAIN LIMITATION
Intervention also increased physical distancing--a major NPI
Authors make a good case why might not matter, but ignores time outside of Mosques, including community transmission in homes
Intervention also increased physical distancing--a major NPI
Authors make a good case why might not matter, but ignores time outside of Mosques, including community transmission in homes
https://twitter.com/Jabaluck/status/1433082231417982978?s=20
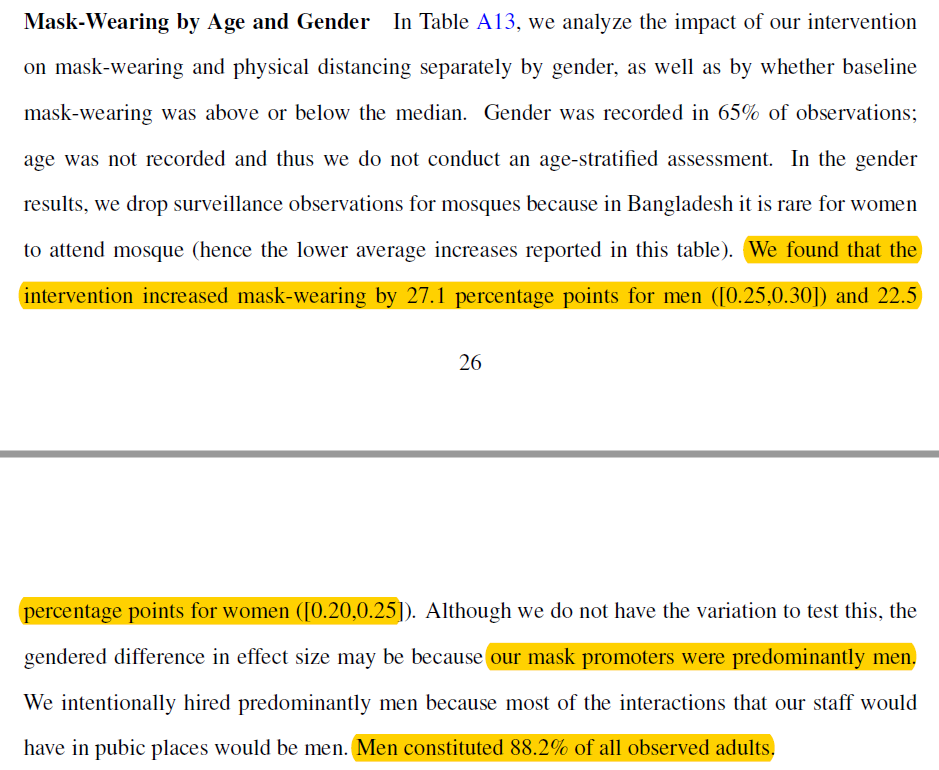
20| LIMITATION CONTINUED
One way to assess if results driven by masks and not distancing because no physical distancing in Mosques is to do a gender subgroup analysis of primary outcome since men & woman in Bangladesh have very different social behaviors
Did I miss this?
One way to assess if results driven by masks and not distancing because no physical distancing in Mosques is to do a gender subgroup analysis of primary outcome since men & woman in Bangladesh have very different social behaviors
Did I miss this?
21| DIRECT TAKE HOME
We can be more surgical (pun intended) in our policy
Really, really, really hard to sustain mask wearing. None of the well thought out interventions worked. For LMIC w/ low vax supply, this is a big challenge
We can be more surgical (pun intended) in our policy
Really, really, really hard to sustain mask wearing. None of the well thought out interventions worked. For LMIC w/ low vax supply, this is a big challenge
22| IMPLICATIONS FOR U.S (& hi income countries)
In areas with high vax (SF) & to some extent high prior infections, benefits of mask will be much smaller
Catch-22 in US is where needed most will have lowest uptake & vice versa (cc SF)
In areas with high vax (SF) & to some extent high prior infections, benefits of mask will be much smaller
Catch-22 in US is where needed most will have lowest uptake & vice versa (cc SF)
https://twitter.com/Jabaluck/status/1433082242960658432?s=20
23| MORE IMPLICATIONS
Agree with authors that more masking and for longer time will increase absolute benefit (why RRR much preferred over ARR here)
But authors ALSO showed how HARD this is, even with well designed interventions & govt support (but no teeth to enforce)
Agree with authors that more masking and for longer time will increase absolute benefit (why RRR much preferred over ARR here)
But authors ALSO showed how HARD this is, even with well designed interventions & govt support (but no teeth to enforce)
24| CAN WE SUSTAIN MASK WEARING?
Unless change in cultural & political beliefs OR mandates with teeth, can't expect repeating intervention will have same effect
Little changed 3 months later!
Same role models & active promotion will tire out
Unless change in cultural & political beliefs OR mandates with teeth, can't expect repeating intervention will have same effect
Little changed 3 months later!
Same role models & active promotion will tire out
25| MY PERSONAL TAKE HOMES
Living in SF, I'm more assured that masks aren't part of long term strategy w/ our incredibly high vax rate, boosters now for high risk, & EUA for children on horizon
Also, my 2 year old shouldn't mask in daycare, esp outdoors in jet turbine SF wind
Living in SF, I'm more assured that masks aren't part of long term strategy w/ our incredibly high vax rate, boosters now for high risk, & EUA for children on horizon
Also, my 2 year old shouldn't mask in daycare, esp outdoors in jet turbine SF wind
• • •
Missing some Tweet in this thread? You can try to
force a refresh