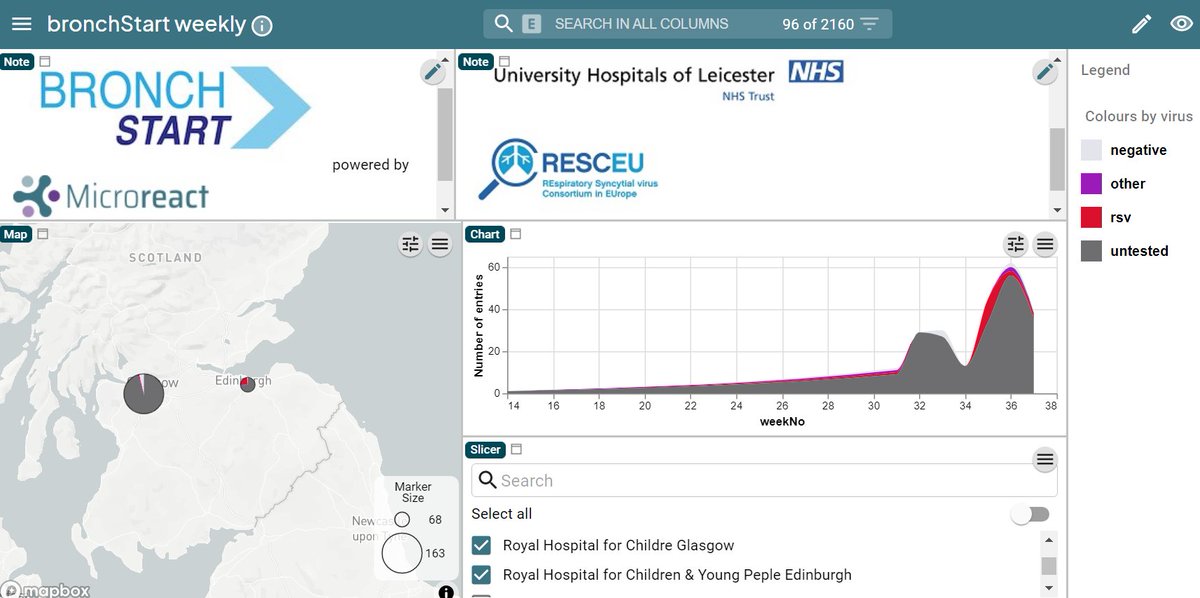
the #BronchSTART study dashboard beta.microreact.org/project/cTkH24… already contains a huge amount of data
and you can see that there have been unusual regional variations in the RSV season this year 🧵 1/n
and you can see that there have been unusual regional variations in the RSV season this year 🧵 1/n
https://twitter.com/Damian_Roland/status/1440412304307154949
normally the RSV season starts in the urban centres of the NW of England and London at around the same time thorax.bmj.com/content/75/3/2… and spreads to the rest of the country in the following 3 weeks 2/n 
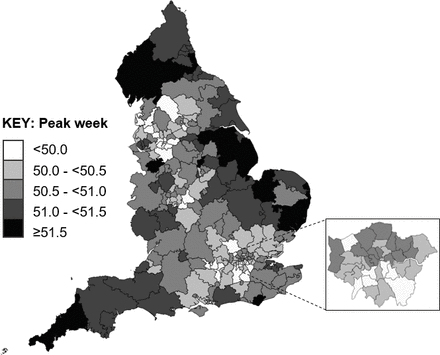
this year, like in previous ones, RSV did start (early? late?) in the urban centres of the NW of England and peaked at epidemiological week 30 3/n

but unlike previous years London lagged behind, so that the peak here was roughly 4 weeks later (week 34) 4/n

meanwhile in Scotland it's not clear whether a peak has been reached or not, with an unusual double peak pattern that it is tempting to ascribe to schools re-starting 5/n
as even more sites come on board, any interested individual or organisation will be able to track RSV spread at high resolution across the UK and Ireland, and find out at a regional level when (if?) case rates start rising again as we move into the autumn/winter 6/n
and find out how our autumn/winter caseload compares to the summer 7/n
with a variety of factors playing into the near future:
- older susceptible population
- influence of schools opening
- climatic variables
- social distancing measures
it is likely that there will be further surprises 8/n
- older susceptible population
- influence of schools opening
- climatic variables
- social distancing measures
it is likely that there will be further surprises 8/n
the hard work of the #BronchSTART @PERUKItweep collaborators (and our dashboard from @MyMicroreact) 9/n
means that we can track these changes in almost real time
and begin to understand some of the factors putting unprecedented pressure on our primary and secondary care colleagues END
and begin to understand some of the factors putting unprecedented pressure on our primary and secondary care colleagues END
• • •
Missing some Tweet in this thread? You can try to
force a refresh