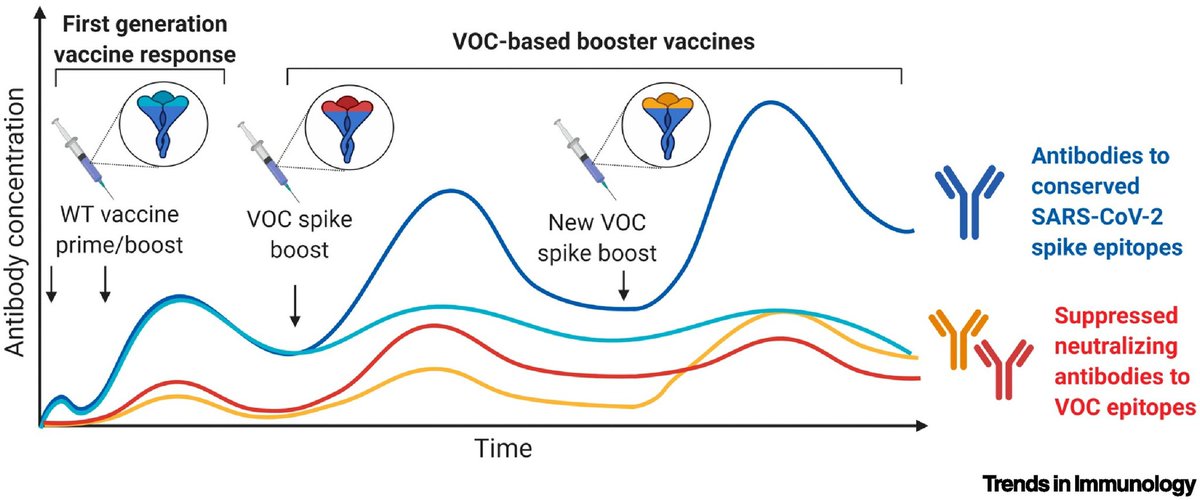
Although there are issues with waning immunity, current COVID-19 vaccines offer excellent protection. But this might not always be the case. Future variant-specific boosters may preferentially boost responses to the original strain and be less effective.🧵
cell.com/trends/immunol…
cell.com/trends/immunol…
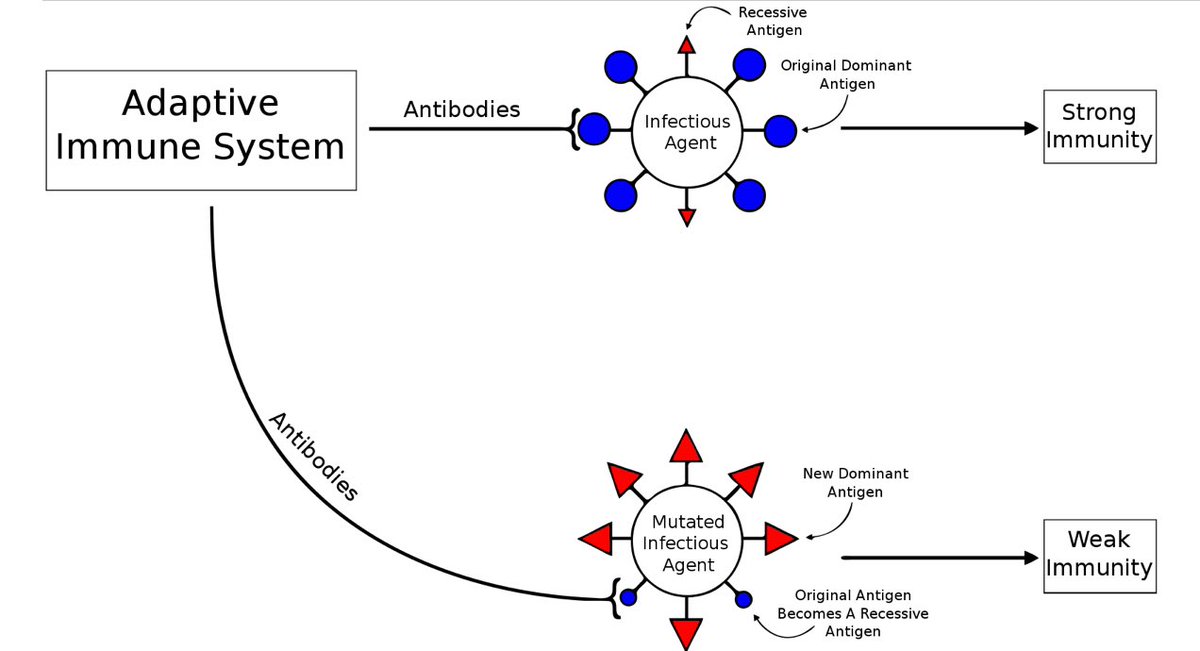
The theory works like this: a person exposed to strain A of the virus (either by vaccination or infection) may prime their immune system such that the ability to make future antibodies specific to a future strain (strain B) is reduced.
This is known as immune imprinting.
This is known as immune imprinting.
In that scenario, a vaccine booster for strain B will give some protection against the new strain B, but the immune system will preferentially produce antibodies against the original strain A.
In certain situations, this has the potential to be harmful.
en.m.wikipedia.org/wiki/Original_…
In certain situations, this has the potential to be harmful.
en.m.wikipedia.org/wiki/Original_…
It is possible that immune imprinting will not turn out to be a significant problem with SARS-CoV-2, and/or it may be possible to design better vaccines that limit this issue.
While the authors of the article linked to at the start of this thread hope that immune imprinting will not be a major problem, they warn that we must take the possibility of future problems seriously.
It’s very important to understand that this is NOT an argument against vaccination.
Immune imprinting also occurs with infection (and you get COVID-19 as well).
Vaccination remains extremely important. Everyone should get vaccinated if they have the opportunity.
Immune imprinting also occurs with infection (and you get COVID-19 as well).
Vaccination remains extremely important. Everyone should get vaccinated if they have the opportunity.
However, we need to think about how we can get the most benefit out of the vaccines we have today.
That means we mustn’t rely on vaccines alone to end the pandemic. We need a #VaccinesPlus strategy: vaccination plus some ongoing (and hopefully unobtrusive) low-level mitigations.
That means we mustn’t rely on vaccines alone to end the pandemic. We need a #VaccinesPlus strategy: vaccination plus some ongoing (and hopefully unobtrusive) low-level mitigations.
We need to use vaccines PLUS things like ventilation improvements in our public buildings.
Improved sanitation was one of the greatest contributors to the increased life expectancy we enjoy today. Nowadays, clean water is taken for granted in most countries.
Improved sanitation was one of the greatest contributors to the increased life expectancy we enjoy today. Nowadays, clean water is taken for granted in most countries.
Today, we need to take the next step and ensure that everyone has access to clean air.
This will reduce transmission of SARS-CoV-2, and also protect us from future pandemics.
This will reduce transmission of SARS-CoV-2, and also protect us from future pandemics.
It’s very unlikely that we will completely eradicate SARS-CoV-2, because the virus has animal reservoirs.
But we can keep transmission to low levels with a #VaccinesPlus strategy.
This will save lives, protect economies, and reduce the risk of new variants emerging.
But we can keep transmission to low levels with a #VaccinesPlus strategy.
This will save lives, protect economies, and reduce the risk of new variants emerging.
By reducing the risk of new variants emerging, we can also lower the risk of running into problems with immune imprinting. This will ensure that we can depend on vaccines to deliver a high level of protection into the future.
• • •
Missing some Tweet in this thread? You can try to
force a refresh