Our paper on vaccination of adolescents co-led with @chrischirp out today in @EditorJRSM. Our risk-benefit analysis of vaccination of adolescents show benefits *far* outweigh risks in reducing deaths, hospitalisations, long COVID at current rates 🧵
rsm.ac.uk/media/5475435/…
rsm.ac.uk/media/5475435/…
What did we do?
We looked at different case incidence rates - continuing for a period of 16 weeks, and looked at how many 12-17 year olds would be hospitalised, be admitted to ICU, develop long COVID or die with and without vaccination during this time in England.
We looked at different case incidence rates - continuing for a period of 16 weeks, and looked at how many 12-17 year olds would be hospitalised, be admitted to ICU, develop long COVID or die with and without vaccination during this time in England.
What rates did we consider?
We reported main results for two rates, but also looked at everything in between.
Our main results are for two case incidences:
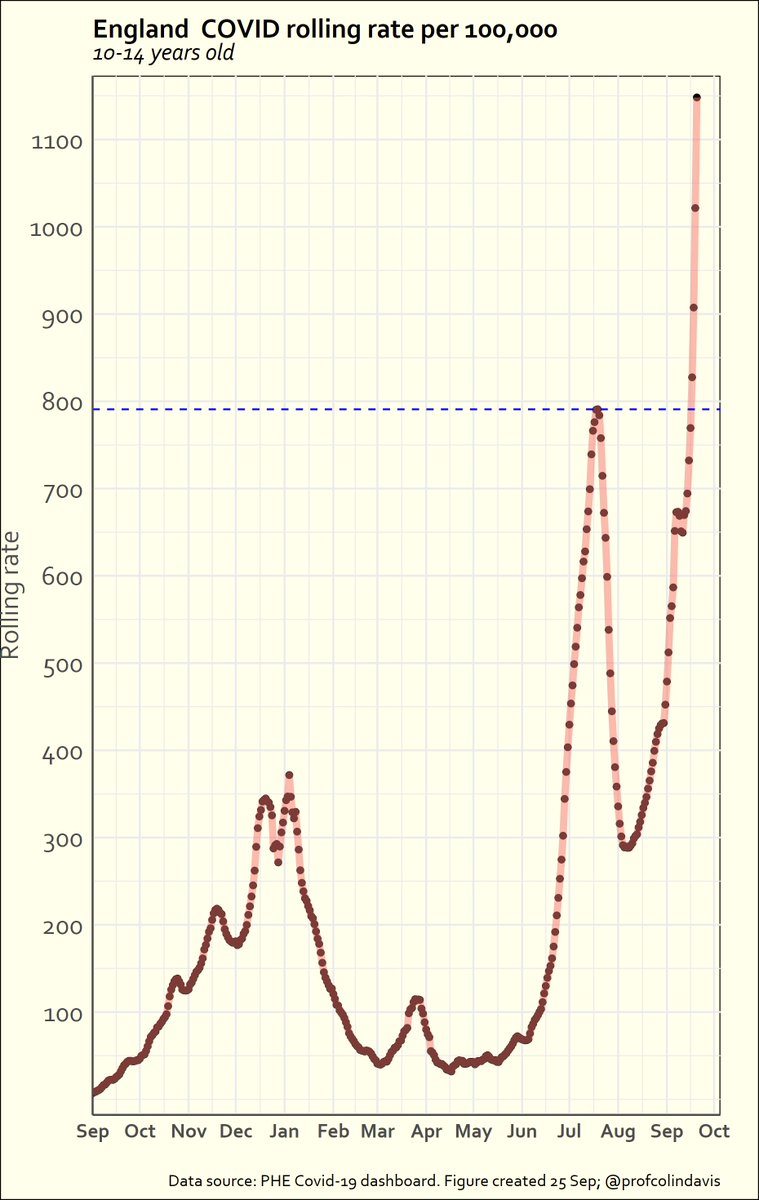
High: 1000/100,000/wk (current incidence in 10-19 yr olds is ~800/100,000/wk for)
Low: 50/100,000/wk (similar to April)
We reported main results for two rates, but also looked at everything in between.
Our main results are for two case incidences:
High: 1000/100,000/wk (current incidence in 10-19 yr olds is ~800/100,000/wk for)
Low: 50/100,000/wk (similar to April)
How did we assess how many would be hospitalised, need ICU admission, die or develop long COVID?
We used linked data from within England from July 2020- 31st March 2021 (we excluded the first wave because children weren't being regularly tested).
We used linked data from within England from July 2020- 31st March 2021 (we excluded the first wave because children weren't being regularly tested).

For myocarditis we considered the rates reported by the FDA/CDC (same as the ones referenced by the JCVI in the table above), and for long COVID we considered 2%, 4% and 14% persistent symptoms at 12 weeks (based on estimates three different studies).
What did we find?
For the high incidence scenario (pretty close to where we are now), the benefits from vaccination are *huge*. Even if we consider that everyone who gets vaccine associated myocarditis is hospitalised, we still prevent 4,600 hospitalisations, and 36 deaths.
For the high incidence scenario (pretty close to where we are now), the benefits from vaccination are *huge*. Even if we consider that everyone who gets vaccine associated myocarditis is hospitalised, we still prevent 4,600 hospitalisations, and 36 deaths.

Even considering 4% of 12-17 years olds get long COVID, we would be preventing 16,000 cases of long COVID. If we consider 14%, this no. is 56,000. If we assume long COVID is rarer (2%) this is 8,000 over 16 wks. No matter how one looks at it the benefits are substantial.
So what if incidence is lower?
If we consider 50/100,000 incidence (>10x lower than current), we still see considerable benefits.
We prevent 230 hospitalisations, 15 admissions to ICU, 2 deaths, and 2,800/800/400 cases of long COVID (14%/4%/2% incidence) over 16 wks.
If we consider 50/100,000 incidence (>10x lower than current), we still see considerable benefits.
We prevent 230 hospitalisations, 15 admissions to ICU, 2 deaths, and 2,800/800/400 cases of long COVID (14%/4%/2% incidence) over 16 wks.

So where does the risk-benefit tilt away from vaccination?
For deaths, and long COVID, it doesn't, because vaccines haven't been associated with any of these - at current incidence we'd be preventing 30 deaths over 16 weeks, and thousands of cases of long COVID.
For deaths, and long COVID, it doesn't, because vaccines haven't been associated with any of these - at current incidence we'd be preventing 30 deaths over 16 weeks, and thousands of cases of long COVID.

For hospitalisations, this balance only tilts at very low incidence rates - so if incidence rates were maintained consistently below ~30/100,000/wk (a rate that hasn't been reached in 2021 at all). So in reality, unless things change *a lot* the benefit always outweighs risks.

But how sensitive are your results to your parameters?
Not very. Even if we assume a lower hospitalisation rate (0.5%) than the one we see in the data in England (0.8%), we still see huge benefits from vaccination unless incidence rates are below 50-60/100,000/wk
Not very. Even if we assume a lower hospitalisation rate (0.5%) than the one we see in the data in England (0.8%), we still see huge benefits from vaccination unless incidence rates are below 50-60/100,000/wk
Let's remember our analyses are likely to be conservative. We assumed 90% protection from severe disease in children, and 64% protection from infection (no additional protection for long COVID). We also only looked at impact over 16 wks - but vaccines have longer term impacts.
Now this bit is for scientist (& other) trolls, so stop reading if you aren't one!
'But you only examined 2 doses, not 1 dose. Why?'
Because there are literally no trials of efficacy & durability 1 dose vaccines in kids or adults. No prizes for guessing why!
'But you only examined 2 doses, not 1 dose. Why?'
Because there are literally no trials of efficacy & durability 1 dose vaccines in kids or adults. No prizes for guessing why!
Almost every other country in the world is giving 2 doses to kids, because it's widely recognised that we don't know enough about protection from a single dose, and we know that in adults two doses are needed for good protection against delta.
But we find that benefits with 2 doses *far* outweigh risks. So if you want to ask about this, perhaps ask JCVI about how they decided on 1 dose, given there is currently no trial data on this. I think those advocating for a single dose need to justify why not the other way round
'You didn't separate out those with pre-existing conditions and 'healthy children'. This means your analysis is useless.'
No, it doesn't. Long COVID happens in all children, including 'healthy' ones, and is common. And 60% of all hospitalisations happen in 'healthy' children.
No, it doesn't. Long COVID happens in all children, including 'healthy' ones, and is common. And 60% of all hospitalisations happen in 'healthy' children.
So benefits in healthy children would be expected to be substantial. Also given vaccine-associated myocarditis apart from being rare has been typically mild and resolved with standard treatment in most cases. But Long COVID hasn't. Why wouldn't you vaccinate 'healthy children'?
And we still don't know which children are most vulnerable to severe disease, and all children are vulnerable to long COVID, so these classifications are unhelpful, and don't help protect children- because all children are unfortunately at risk from infection.
We also didn't assess impact on reduction in educational disruption, and transmission to household members (including vulnerable household members). Adding these on would only add to the benefits of vaccination- including in 'healthy children'.
I'd hope scientists and journalists would be as interested in asking JCVI how they did their calculations, given they've actually informed policy, and public messaging, and still not been published 4 wks after release. Ours are peer-reviewed and open for anyone to scrutinise.
• • •
Missing some Tweet in this thread? You can try to
force a refresh