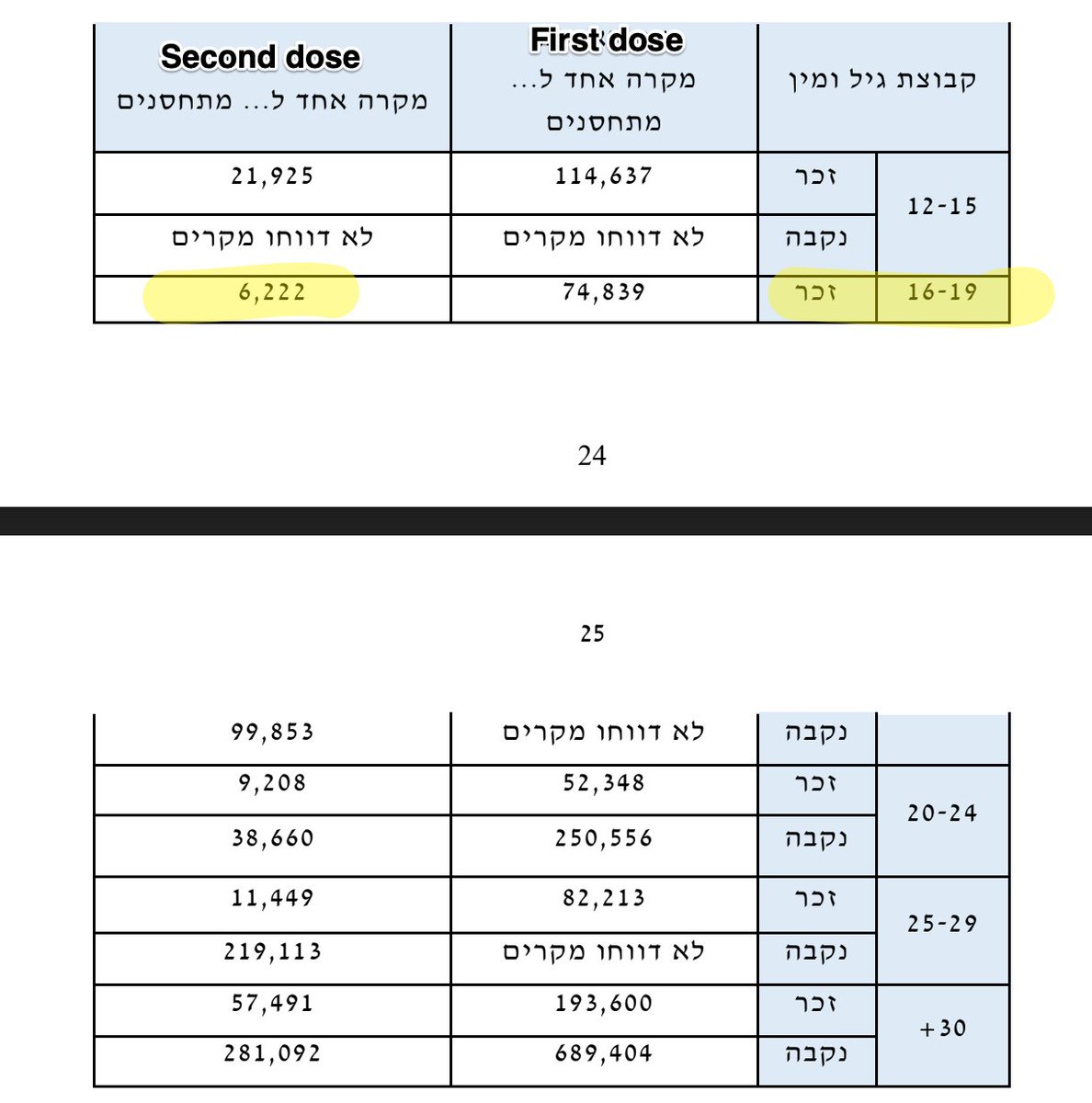
The Israeli @nejm study published today that stratified for myocarditis rates post vax dose 2 in males age 16-19 found a rate of 1/6600 for Pfizer. Our preprint found a *lower* rate of 1/10,600 for 16-17 yo males. For 12-15 yo males we found 1/6200 nejm.org/doi/full/10.10…
I'm really grateful for this NEJM study⬆️ & glad to see our VAERS-based study didn't provide an overestimate in 16-17 yo males. This was as expected with VAERS typically underreporting. I hope more studies are published with 12-15 year old estimated rates. medrxiv.org/content/10.110…
From second NEJM study "Most cases of myocarditis were of mild or intermediate severity" "1 patient had cardiogenic shock, & 1 patient w/preexisting cardiac disease died of an unknown cause after.. discharge Left ventricular dysfunction in 29% of patients" nejm.org/doi/full/10.10…
Even in young males this condition is RARE & mostly benign, but discussions like this are important:
@walidgellad quoted: “Parents who are hesitant may appreciate the fact that the risk of side effects is... much lower for 1 dose than it is for 2 doses.”
nytimes.com/2021/10/06/hea…
@walidgellad quoted: “Parents who are hesitant may appreciate the fact that the risk of side effects is... much lower for 1 dose than it is for 2 doses.”
nytimes.com/2021/10/06/hea…
I would just add one more thing though that, as we said in our pre-print based on data from Ontario and, given the news from Scandinavia, the rates from Moderna may be around 2 fold higher than these reported rates from Pfizer. medrxiv.org/content/10.110…
Finally, I am very pro vax and encourage any unvaccinated patients I see to get vaccinated but in the demographic of young boys w/mRNA vax we need a proper risk benefit analysis that considers 1 dose and the benefits of natural immunity.
• • •
Missing some Tweet in this thread? You can try to
force a refresh