1/ Future of Obesity Treatments? #OW2021
Meet the candidates:
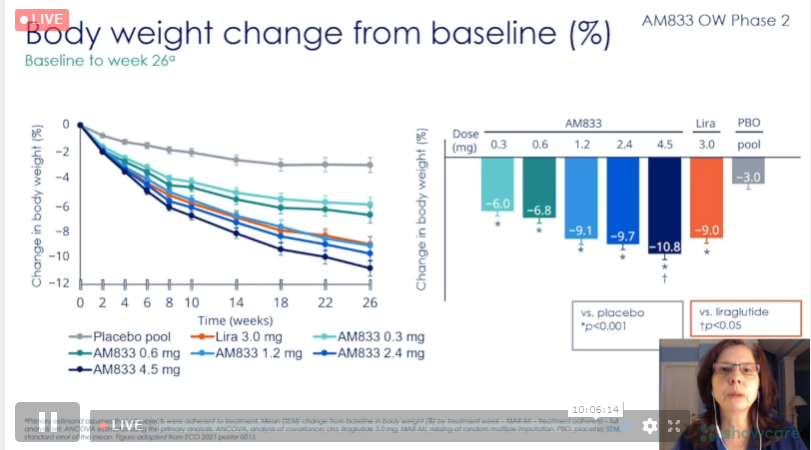
1) AM833 +/- Semaglutide 2.4 mg; combo therapy resulted in 15-17% at 20 weeks with no evidence of nadir, suggesting even greater wt loss (likely >20%).
by Dr. Rubino
Meet the candidates:
1) AM833 +/- Semaglutide 2.4 mg; combo therapy resulted in 15-17% at 20 weeks with no evidence of nadir, suggesting even greater wt loss (likely >20%).
by Dr. Rubino


2/ Tirzepatide; hard to imagine a future without tirzepatide (as long as safety & tolerability remain) for the treatment of metabolic dz when >10% wt loss and -2.5% A1c are avg results. Also, >50% of participants achieved normoglycemia with most doses‼️
↪️by Dr. Frias #OW2021
↪️by Dr. Frias #OW2021




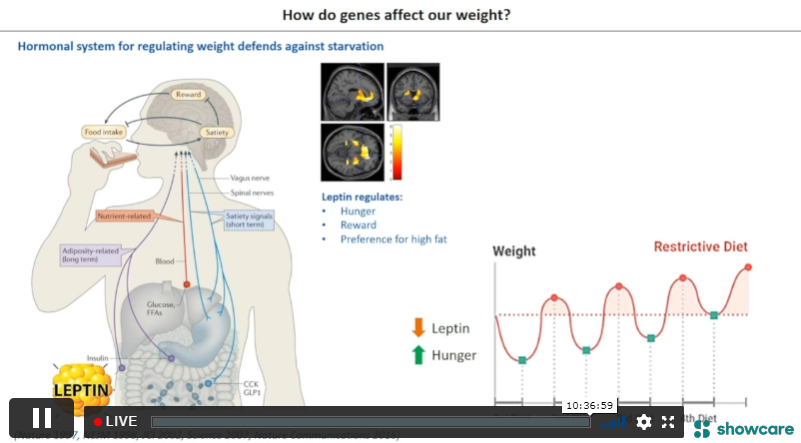
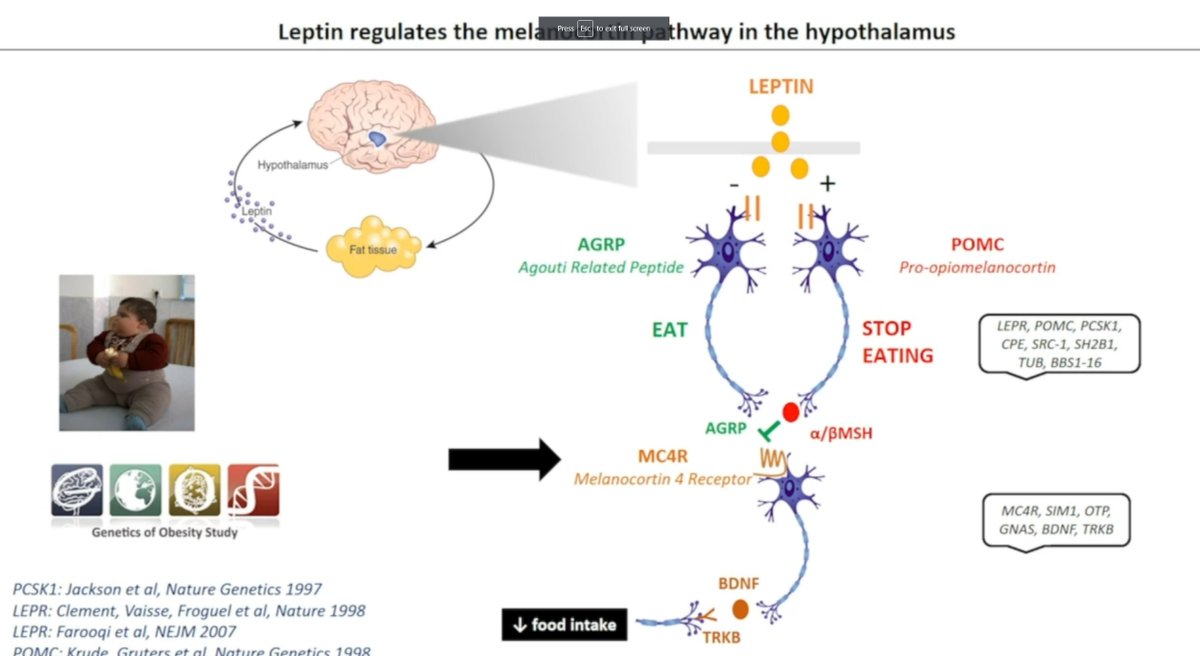
3/ Setmelanotide; MC4R agonist targets central POMC/MC4R pathway in hypothalamus. Currently reserved for congenital obesity.
➡️ 1 in 300 carry MC4R loss of fxn variant (predisposes to wt gain)
➡️ 6 in 300 carry MC4R GoF variant that protects against wt gain
↪️ by @Farooqi_Lab
➡️ 1 in 300 carry MC4R loss of fxn variant (predisposes to wt gain)
➡️ 6 in 300 carry MC4R GoF variant that protects against wt gain
↪️ by @Farooqi_Lab

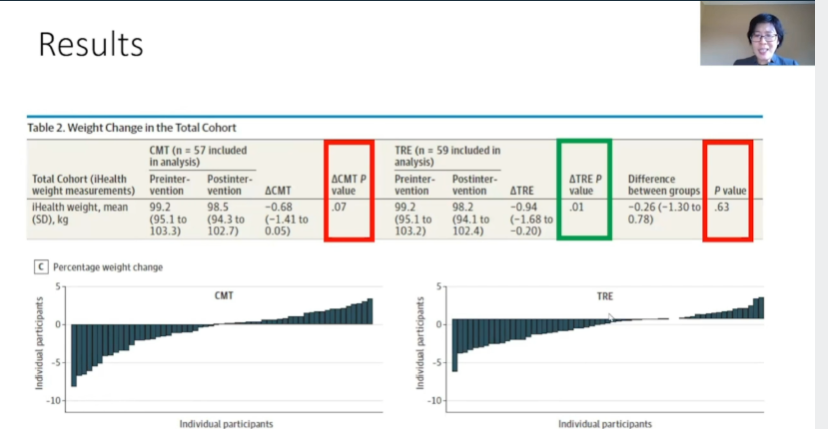
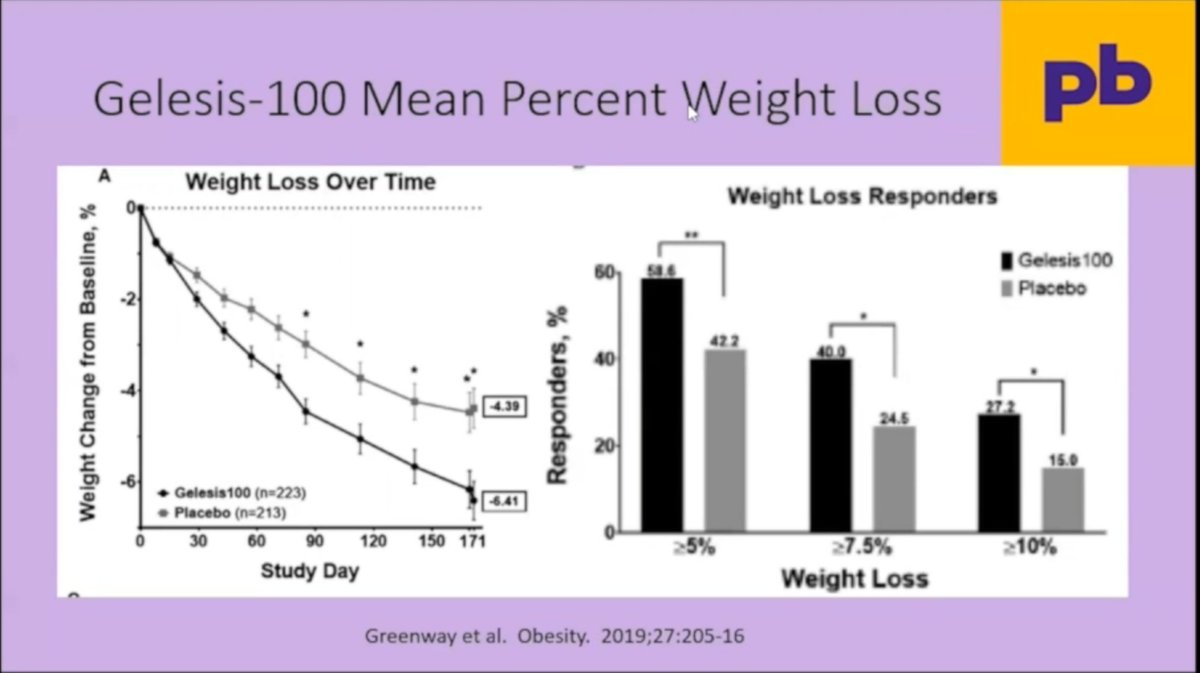
4/ Oral Superabsorbent Hydrogel
➡️ Gel is biodegradable and food-grade quality
➡️ Avg wt loss >5% with >25% achieving at least 10% or more WL. Works best for ppl with impaired glucose tolerance (Pre-DM/DM2)
➡️ Broadest indication for treatment: BMI 25-40
↪️Dr. Greenway #OW2021
➡️ Gel is biodegradable and food-grade quality
➡️ Avg wt loss >5% with >25% achieving at least 10% or more WL. Works best for ppl with impaired glucose tolerance (Pre-DM/DM2)
➡️ Broadest indication for treatment: BMI 25-40
↪️Dr. Greenway #OW2021

5/ Bimagrumab; monoclonal antibody against activin type II receptors (ActRII)
➡️ remarkable changes in body composition (⬆️ lean mass, ⬇️ fat mass)
➡️ remarkable changes in body composition (⬆️ lean mass, ⬇️ fat mass)



interesting, that bimagrumab led to significant increases in hs-CRP. No one knows why? I would consider this concerning. 🤔
• • •
Missing some Tweet in this thread? You can try to
force a refresh