Great to be at an in person médical conference, on Alzheimers disease, in Boston. This particular conference was founded in 2008.
Quite some excitement that we are now in the therapeutic era for AD.
But so striking the conference kicked off by a panel of old men.
/1
Quite some excitement that we are now in the therapeutic era for AD.
But so striking the conference kicked off by a panel of old men.
/1


It is notable how the leaders of the field haven't really changed in 13 years. Some have died of course. But leadership seems very unrepresentative of the research base.
It is about time conference organizes avoided keynote panels limited to old white men.
/2
It is about time conference organizes avoided keynote panels limited to old white men.
/2
And we now get @jasonkarlawish who has criticised the FDA accelerated approve of aducanumab.
"we have set a new standard [for approval] that people don't quite believe in".
He is speaking remotely. Hopefully not because he would have felt uncomfortable here.
"we have set a new standard [for approval] that people don't quite believe in".
He is speaking remotely. Hopefully not because he would have felt uncomfortable here.

Killer audience question
"two years after the [aducanumab] results were presented at this conference we still haven't seen a peer reviewed publication".
No response from panel. Absolute silence from the audience.
Quite a moment.
/4
"two years after the [aducanumab] results were presented at this conference we still haven't seen a peer reviewed publication".
No response from panel. Absolute silence from the audience.
Quite a moment.
/4
Another killer question from a former senior executive at Pfizer.
"we have learned the hard way to do things a certain way that were not done in this case [aducanumab]. For example the need for replication" (biogen did not have 2 pivotal trial that met primary endpoints).
/5
"we have learned the hard way to do things a certain way that were not done in this case [aducanumab]. For example the need for replication" (biogen did not have 2 pivotal trial that met primary endpoints).
/5
"I am sorry there a no further time for questions"
Dry laughter from the audience.
Really tense atmosphere after those questions from the audience.
À seriously y controversial decision by FDA.
/6
Dry laughter from the audience.
Really tense atmosphere after those questions from the audience.
À seriously y controversial decision by FDA.
/6
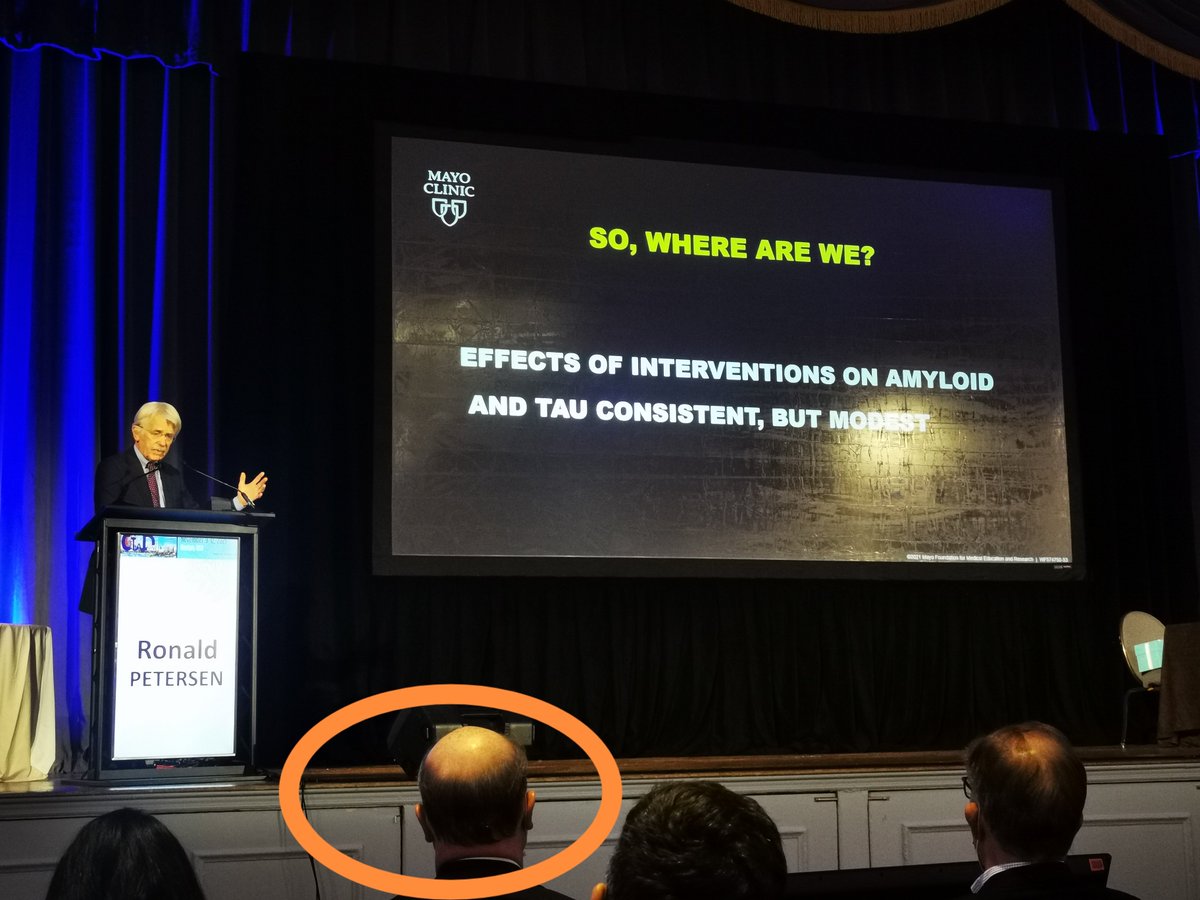
And it was impressive that the FDA's Billy Dunn who has received a lot of criticism for his division's decision on aducanumab, was in the front row during the session.
(circled)
/7
(circled)
/7
• • •
Missing some Tweet in this thread? You can try to
force a refresh